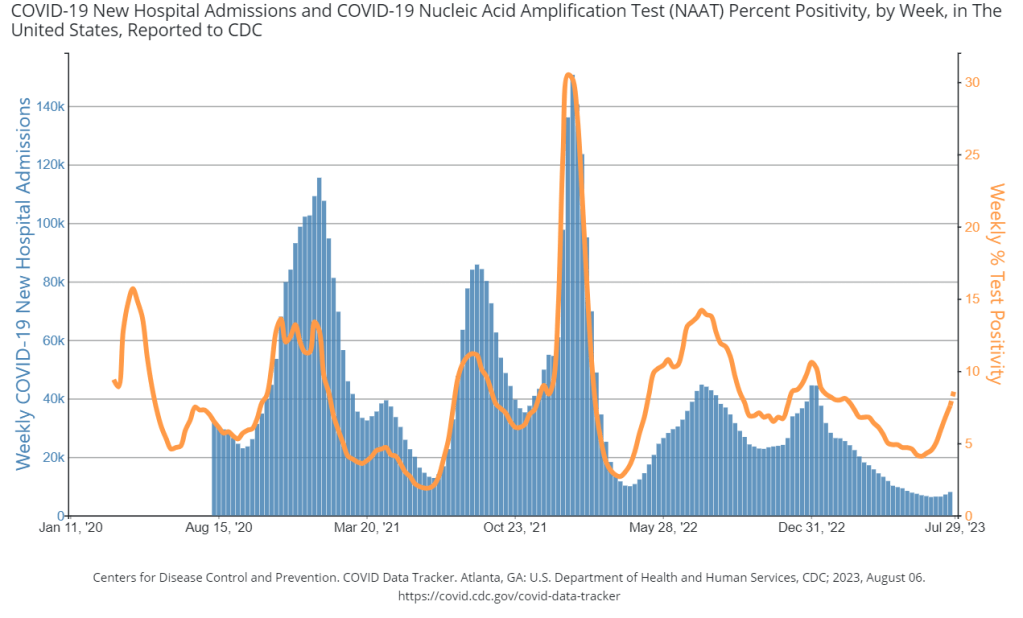

During the most recent week of data available (July 23 through 29), the U.S. reported about 9,000 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
- An average of 1,300 new admissions each day
- 2.8 total admissions for every 100,000 Americans
- 13% more new admissions than the prior week (July 16-22)
Additionally, the U.S. reported:
- 10.6% of tests in the CDC’s surveillance network came back positive
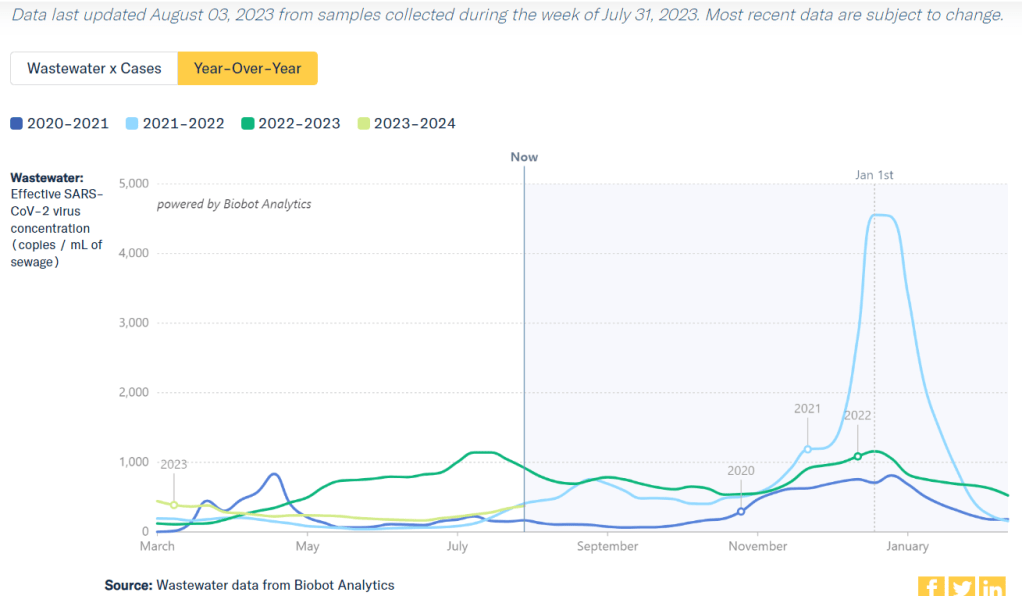
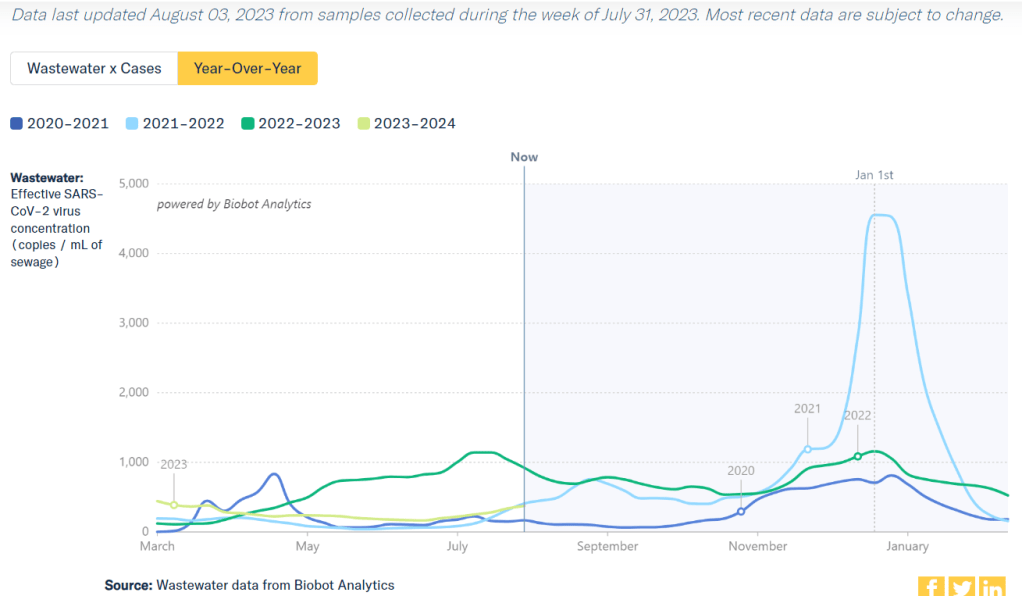
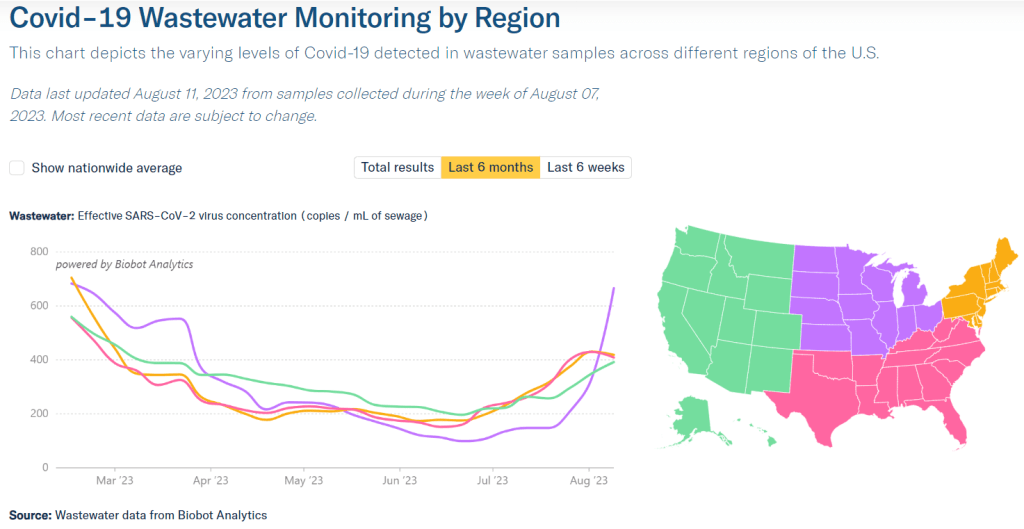
- A 9% higher concentration of SARS-CoV-2 in wastewater than last week (as of August 9, per Biobot’s dashboard)
- 31% of new cases are caused by Omicron XBB.1.6; 17% by EG.5; 11% by XBB.2.3; 10% by XBB.1.9 (as of August 5)
All major COVID-19 metrics continue to increase in the U.S., as we deal with a late-summer surge. Wastewater surveillance suggests that current virus spread is on pace with the Delta surge in 2021, though other data sources are less reliable these days.
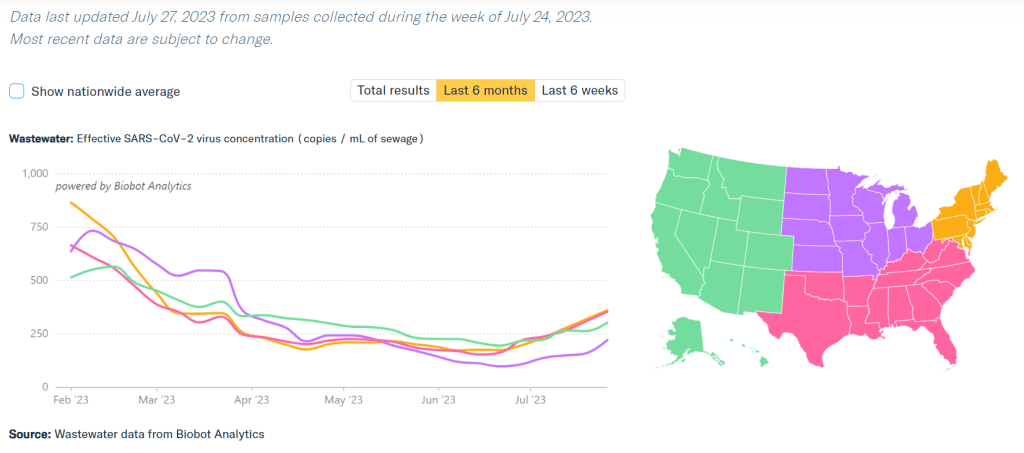
Wastewater data from Biobot continue to show an uptick nationally, following the same upward trend that started in late June. The CDC’s wastewater surveillance system and WastewaterSCAN network report similar trends.
Biobot’s regional data suggest that the Northeast and South, the first two regions to see COVID-19 increases this summer, might be approaching their peaks, but it’s too early to say for sure. Regional test positivity numbers, from the CDC, show no sign of slowing their rise.
Meanwhile, COVID-19 spread is going way up in the Midwest, per Biobot and WastewaterSCAN. Some sewersheds in Iowa, Michigan, Ohio, and nearby states have reported their viral levels in wastewater more than doubling over the last couple of weeks.
Test positivity nationwide is now over 10%, per the latest data from the CDC’s respiratory virus testing network. Walgreens’ COVID-19 dashboard, which displays testing data from its pharmacies (i.e. a smaller sample size than the CDC network), reports a record high: of about 2,400 COVID-19 tests conducted in the week ending August 6, 45% were positive.
Hospital admissions for COVID-19 are also on the rise, with about 1,300 new hospitalizations for COVID-19 each day in the week ending July 29, per the CDC. While it’s true that these numbers are far lower than peaks during prior surges, the data are also less reliable now— with fewer hospitals reporting to the CDC and fewer measures in those hospitals (like masking) to control infections.
A lot of articles in the last couple of weeks have connected the recent surge to EG.5, the latest Omicron subvariant gaining ground in the U.S. However, this variant is not necessarily causing the surge; it doesn’t seem to be meaningfully more contagious or more severe than other recent strains, scientists are finding.
Rather than a variant, I would personally attribute this surge to summer travel and gatherings, combined with waning immunity—it’s been many months since most Americans had contact with the virus through vaccination or infection.
All of the virus-spreading activities going on right now will give SARS-CoV-2 more avenues to mutate. And there are other variants circulating globally that could cause more problems in the U.S. as well, as Eric Topol outlines in a recent Substack post. The next booster can’t come soon enough.