The CDC expects that our next round of COVID-19 booster shots will be available in early fall, likely late September or early October. But this limited information has been distributed not through formal reports or press releases—rather, through the new CDC director’s media appearances.
These booster shots will be targeted to Omicron XBB.1.5, one of the most recently-circulating subvariants. It’ll be an important immunity upgrade, especially for seniors and other higher-risk people, as the last round of updated vaccines came almost a year ago. Plus, these new boosters are basically the federal government’s one initiative to combat COVID-19 as we head into another inevitable fall and winter of respiratory illness.
Considering the shots’ importance, we have surprisingly little information about when they’ll be available or how they will be distributed. During one media appearance (on NPR’s All Things Considered in early August), CDC Director Dr. Mandy Cohen said that the boosters would be available “probably in the early October time frame.” Then, a week later (on former federal official Andy Slavitt’s podcast), she said boosters would come “by the third or fourth week of September.”
In both interviews, Cohen shared few details beyond this vague timeline. I would love to see more details from the federal government about their plans—for producing the shots, and also for distributing them in our post-federal emergency landscape. It also seems unclear how the CDC and other agencies will promote the boosters, considering how most officials are now pretending COVID-19 is no longer a concern. (Case in point: Cohen’s many mask-less appearances since she started as CDC director.)
This past Thursday, the FDA’s advisory committee on vaccines and similar biological products met to discuss COVID-19 boosters for this fall. They voted in favor of updating the vaccines based on Omicron XBB, a variant lineage that has dominated both in the U.S. and globally this year.
The fall boosters will be monovalent, meaning they’ll only include the XBB strain—unlike our most recent boosters, which were bivalent (including BA.4/BA.5 and the original, Wuhan strain). The FDA has recommended this switch because research suggests monovalent vaccines may be more effective, and because the original coronavirus strain is no longer circulating; we’re mostly seeing XBB right now.
The FDA has not yet decided which exact variant will be used for this fall’s boosters. While experts generally agree that it should be an XBB lineage, the FDA will make a final call on this closer to the fall respiratory virus season. XBB.1.5, XBB.1.9, and XBB.1.16 are all major contenders right now.
This fall’s vaccination campaign is likely to prioritize at-risk populations, including seniors and those with medical conditions that damage their immune systems, similar to the bivalent booster shot rollouts. Ongoing vaccine effectiveness research suggests that these groups benefit most from the protection of an additional booster shot, though people not in these groups obviously benefit as well.
The CDC will make final decisions about which groups will most need the fall boosters, as well as whether some groups may be eligible for more than one of the shots. Children may also become eligible for new boosters; that’ll be up to the CDC as well.
In choosing XBB for the fall boosters, the FDA is standardizing with recommendations from the World Health Organization and European Union, which have also suggested that XBB be the target for the next boosters. Last year, the WHO recommended BA.1, while the U.S. used BA.4/BA.5. Standardizing will be helpful for ongoing data collection, since…
Data problems persist: I’ve written a lot about the U.S.’s disadvantages in tracking vaccine effectiveness, particularly compared to other countries with more standardized health systems. This problem has persisted through all rounds of boosters, including the shots planned for this fall; in fact, it’s even harder now for U.S. agencies to monitor how well the vacines work, as the federal public health emergency’s end led to fewer data collection authorities for the CDC. (Safety monitoring systems will continue, though.)
It’s also worth noting that the boosters this fall will be the first major COVID-19 vaccine rollout following the end of the federal public health emergency. While the Biden administration has devoted some funding for getting vaccines to uninsured Americans, most people will now be getting vaccinated through their health insurance.
This is certain to make the process more complicated and more challenging for many. I’ve already seen stories of people who are eligible for a second bivalent booster having a hard time getting that shot. (See this recent Death Panel episode, for example.) The federal government is doing very little to improve this situation in time for the fall boosters to arrive—and no matter how well XBB vaccines work in theory, they’ll do little in practice if nobody can actually get them.
New Long COVID papers from the Patient-Led Research Collaborative: Speaking of new Long COVID research: the Patient-Led Research Collaborative, a group of long-haulers who do and support research on their condition, has recently published two new papers. The first, published in Nature and based on a patient survey, discusses Long COVID’s intersection with common psychiatric conditions such as depression and anxiety. The second, published in Fronteirs in Rehabilitation Science,is a review paper going over the reproductive health impacts of Long COVID. Long COVID frequently causes disruptions to the menstrual cycle, gonad function, fertility, and other areas of reproductive health, yet these symptoms are understudied.
FDA fully approves Paxlovid: The FDA has provided full approval to Pfizer for its antiviral COVID-19 pill, Paxlovid. Millions of Americans have received Paxlovid since it earned Emergency Use Authorization in late 2021, and many studies have shown that it’s effective in reducing the risk of severe COVID-19 symptoms. With the federal public health emergency’s end, the FDA has encouraged pharmaceutical companies to apply for full approval for their COVID-19 products so that they can permanently remain on the market; Paxlovid is a high-profile example of that trend.
Bivalent COVID-19 vaccines protect, but wane: The CDC published another study this week evaluating the bivalent (or Omicron-specific) COVID-19 booster shots. These vaccines clearly provide additional protection against severe COVID-19 symptoms, the study finds, but this immune system boost goes away after several months. In the study, vaccine effectiveness against hospitalization declined from 62% in early weeks post-vaccination, to 24% at three to six months post-vaccination. The study shows that additional boosters and/or newer vaccines are needed for vulnerable adults.
Value of regular testing for controlling outbreaks: Another notable new study: researchers at the University of Wyoming compared how well different mitigation strategies work for preventing the spread of COVID-19 and other diseases, using a model informed by both epidemiological and economic factors. They found that frequent testing—paired with isolation for people who tested positive—was more effective at reducing disease spread than physical distancing measures, like closing businesses or having employees work from home. The paper suggests that testing can help reduce illness while keeping businesses open.
Funding for a WHO disease surveillance initiative: The Rockefeller Foundation and World Health Organization recently announced a new partnership, with the foundation providing $5 million to support the WHO’s Hub for Pandemic and Epidemic Intelligence. This Hub was established in 2021, with goals including fostering global collaboration on disease surveillance, providing better (and more complete) data, and improving tools for public health decisions. Rockefeller’s support will help with scaling up genomic surveillance, real-time data collection, and more.
New funding from CDC’s forecasting center: The CDC’s Center for Forecasting and Analytics (CFA) announced a new funding opportunity for state and local health agencies to develop new disease modeling tools. CFA is a relatively new center itself; it launched last year with the goal of modernizing the U.S.’s disease forecasting capacities (see my FiveThirtyEight article about the center for more details). This funding opportunity will, I expect, enable the CFA’s growing staff to work directly with health agencies on advancing analytical methods. I look forward to seeing the results of those projects.
Experts argue to keep masks in healthcare: A new commentary article, published this week in the Annals of Internal Medicine, argues in favor of keeping mask requirements in healthcare settings. The experts (from the National Institutes of Health and George Washington University) point to real-world experience, suggesting transmission between patients and healthcare workers is less likely when everyone is wearing a mask, preferably one of high quality. This article coincides with an advocacy campaign to keep masks in healthcare, including virtual and in-person actions across the U.S.
CDC releases provisional drug overdose data for 2022: The CDC’s National Center for Health Statistics has released overdose data for 2022, reporting that nearly 110,000 Americans died of overdoses for the second year in a row. Overdoses have leveled off from 2021, but the 2022 data still represent a sharp increase from pre-pandemic trends. Some states in the South and West Coast (such as Texas, Oklahoma, Wyoming, Washington) saw the sharpest increases from 2021 to 2022, according to the CDC. These data are all preliminary and will be updated later in the year.
Pediatric COVID-19 boosters could save school days: A new modeling study, published this week in JAMA Network Open, suggests that the U.S. could have seen about 10,000 fewer kids hospitalized with COVID-19 and 5.5 million fewer school days lost during the 2022-2023 respiratory virus season, if kids received booster shots in large numbers. The researchers arrived at these estimates through a model that simulated COVID-19 booster vaccination rates at similar levels to annual flu vaccination in kids. Future booster campaigns should focus on children in addition to older adults, the authors argue.
RSV vaccine for infants moves ahead: Speaking of pediatric vaccinations: the FDA’s vaccine advisory committee met last week to discuss a new vaccine candidate from Pfizer, which would protect infants from RSV. Unlike most pediatric vaccines, this shot would be delivered to pregnant parents in order to protect their babies at birth. While the FDA’s advisors endorsed the vaccine for its effectiveness, some committee members expressed concerns over safety. Helen Branswell at STAT has more details.
KFF Medicaid Unwinding tracker: The Kaiser Family Foundation just published a new tracker detailing Medicaid enrollment by state. Enrollment rose to record levels during the pandemic, as a federal measure tied to the public health emergency forbid states from taking people off the insurance program. Now, states are going through the slow process of evaluating people’s eligibility and taking some off the program, in a process called “unwinding.” The KFF tracker is following this process, presenting both Medicaid enrollment data by state and information on each state’s timeline for evaluation.
Biden administration ends vaccine mandates: In time with the federal public health emergency’s end, the Biden administration has announced that it will lift its COVID-19 vaccine rules for federal workers and contractors. International travelers to the U.S. also will no longer need to provide proof of their vaccination status, and the administration is working to end requirements for other groups of workers and travelers. This change is, essentially, another signal of the administration giving up on mass vaccination campaigns; after all, most of the people who got their shots under these rules haven’t received an Omicron booster.
Vaccine protection wanes over time: A new review paper from researchers in Trento, Italy, published this week in JAMA, shows the importance of booster shots for maintaining protection from COVID-19. The researchers compiled and analyzed findings from 40 studies that evaluated vaccine effectiveness. Overall, they found, the protection that both primary series and booster shots provide against an Omicron infection drops significantly by six months and nine months after vaccination. Remember: Americans over 65 and/or immunocompromised, you’re now eligible for another bivalent/Omicron-specific booster.
Disparities in COVID-19 deaths persist: Two new studies this week examine COVID-19 deaths by race and ethnicity. The first study, from the CDC’s National Center for Health Statistics, examined deaths of all causes during the pandemic, finding that Black and Native Ameircans had higher death rates than other racial/ethnic groups. COVID-19 was the fourth highest cause of death in 2022, after heart disease, cancer, and unintentional injury. The second study, from Andrew Stokes and collaborators, examined COVID-19 deaths during the U.S.’s first Omicron wave compared to earlier surges, finding that disparities decreased—but only because white deaths went up during the second year of the pandemic.
Characterizing Long COVID neurological symptoms: Another new study from this week: researchers at the NIH performed detailed examinations of 12 Long COVID patients to better understand their neurological symptoms. The researchers used an approach called “deep phenotyping,” which involves a variety of tests that aren’t typically used in clinical settings. They found that the patients had a number of abnormalities in their immune systems and autonomic nervous systems compared to healthy controls, pointing to different potential drivers of symptoms.
FDA approves RSV vaccine: Finally, a bit of non-COVID good news: for the first time, the FDA has approved a vaccine for RSV, the seasonal respiratory virus that can cause severe symptoms in older adults and young children. This vaccine, made by GSK, was approved for adults ages 60 and up and will likely get distributed during the next cold/flu season. Scientists have been working on RSV vaccines for decades, making this a major milestone for reducing the disease’s impact. Helen Branswell at STAT has more details.
External review of the CDC: The People’s CDC, a group of public health experts, scientists, and educators dedicated to advocating for increased COVID-19 precautions, released a new report reviewing the federal CDC’s actins during the pandemic. The report incorporates feedback from a survey of almost 500 experts and from over 200 reports. Overall, the People’s CDC “found that the CDC has prioritized individual choice and short-term business interests over sharing accurate scientific evidence with the public and protecting population health.” (Disclaimer: I was one of the experts surveyed for this report!)
Use of COVIDTests.gov: This new paper, published in the CDC’s Morbidity and Mortality Weekly Report (MMWR), reports on how Americans used COVIDTests.gov, the USPS/HHS effort to distribute free at-home tests. Since the site’s launch in January 2022, about one in three U.S. households received a test kit from this program, the research team found. They also found that this program may have helped improve equity in COVID-19 test access, as Black and white Americans utilized the free tests at similar rates. Of course, the program has been discontinued as of this spring.
Impact of racial discrimination on vaccination: Speaking of health equity: another report published in MMWR this week shares a correlation between discrimination and vaccination status. Researchers at the CDC and their collaborators analyzed data from the CDC’s National Immunization Survey, including about 1.2 million survey results from April 2021 through November 2022. Among the respondents, people who reported experiencing racial or ethnic discrimination in a healthcare setting were less likely to be vaccinated for COVID-19. The findings confirm many health experts’ equity concerns from early in the vaccine rollout.
Declining childhood vaccinations worldwide: Vaccine equity is a concern on the global scale, too. A new report from UNICEF shows that 67 million children worldwide missed at least one vaccination between 2019 and 2021, as healthcare systems were strained. The report also presents new data on global confidence in childhood vaccines: in some countries, this confidence has dropped by up to 44 percentage points. Vaccine confidence only improved in three countries (China, India, and Mexico). “The threat of vaccine hesitancy may be growing,” UNICEF warns.
Healthcare workers present while sick: One more paper that caught my attention this week: researchers at the Veterans Affairs healthcare system in Boston tracked a cohort of about 4,000 healthcare workers between December 2020 and September 2021. In addition to PCR testing, the workers conducted daily COVID-19 symptom reviews, and received guidance to stay home or leave work if they didn’t feel well. But the researchers found that many workers didn’t actually stay home: among 255 workers who had symptomatic COVID-19 during the study period, almost half reported that they were present, at work, at the time they received a positive test result. The paper indicates why it’s important to keep masks in healthcare settings, even when community cases are lower.
This week, the FDA made some adjustments to the U.S.’s COVID-19 vaccine guidance in order to standardize all new mRNA shots to bivalent (or Omicron-specific) vaccines, and to allow adults at higher risk to receive additional boosters. The CDC’s vaccine advisory committee and Director Rochelle Walensky both endorsed these changes.
Adults are now considered “up to date” on their COVID-19 vaccines if they have received at least one dose of a bivalent/Omicron-specific vaccine. These are the vaccines manufactured by Pfizer and Moderna that became available last fall.
Any unvaccinated adult should receive one dose of a bivalent vaccine, rather than the former primary series (which was based on the original coronavirus strain). The prior vaccines will essentially go out of use in the U.S.
Seniors (65 or older) and immunocompromised adults may receive an additional bivalent vaccine dose, starting at four months after their prior dose. Recent research has demonstrated that protection from these shots wanes over a couple of months, so there’s a good case for seeking out a new booster if you fall into one of these high-risk categories.
Immunocompromised adults may receive more bivalent doses going forward, in consultation with their doctors. This guidance intends to provide more protection to people who are severely immunocompromised, such as those undergoing cancer treatment.
A new version of the bivalent booster will likely be available in the fall, designed to protect against more recent coronavirus variants. We don’t know much about this yet, but prior FDA and CDC meetings have suggested it will roll out on a similar schedule to the annual flu shot.
These recommendations mostly apply to adults. While the FDA and CDC are also working on simplifying their guidance for children (to similarly prioritize vaccines aligned to current variants), that’s still a more complicated situation right now. See the YLE post for more details.
Another open question, at the moment, is what non-mRNA vaccines may be available, for people who may be allergic to those vaccines or who had severe reactions to earlier doses. Novavax is reportedly working on a bivalent/Omicron-specific option, which people might be able to get this fall. The Johnson & Johnson vaccine is no longer widely used at all.
It makes sense for the FDA and CDC to shift towards bivalent vaccines. Numerous studies have demonstrated that these vaccines perform better against Omicron variants, and this move simplifies the immunization process for everyone involved (doctors, pharmacies, patients, etc.).
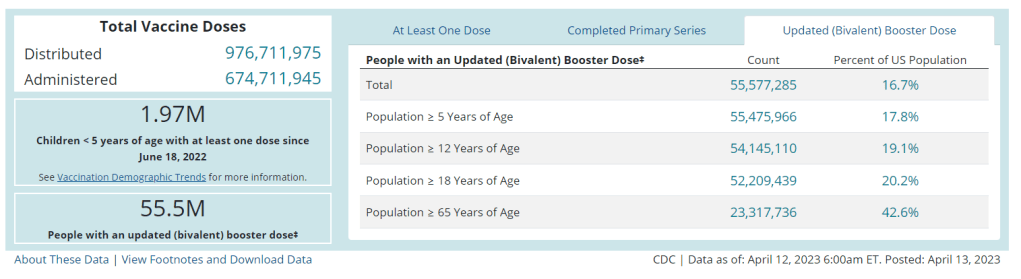
However, this shift reveals how poorly the bivalent booster rollout has gone in the U.S. so far. Only 17% of the population has received one, compared to 81% who’s received at least one dose overall, according to the CDC. Even among seniors, only 42% have received a bivalent booster. It would be a massive task for the country to move towards “up-to-date” coverage among all adults.
And the federal government doesn’t appear to be pushing for this in any meaningful way. I’ve already seen several reports on social media of people trying to get an additional booster, and failing—whether because of an insurance issue or because pharmacies have simply stopped offering the shots. This process will only get more challenging when the federal public health emergency ends next month. While the Biden administration has announced funding to cover vaccines for uninsured Americans, that’s just one hurdle among a growing number.
Low uptake of the Omicron-specific boosters does not inspire confidence in the government’s ability to distribute next-gen vaccines. Data from the CDC.
This week, the White House announced that it’s setting up a $5 billion program to support next-generation COVID-19 vaccines and treatments. The program, called Project Next Gen, is essentially a follow-up to Operation Warp Speed (which launched our current COVID-19 vaccines in 2020).
Project Next Gen is a big step toward actually ending the pandemic, not just pretending it’s over. The federal government can support large-scale clinical trials and speed up regulatory approval in a way that no research group or company could. Still, the U.S.’s prior vaccine campaigns don’t inspire confidence that this project will lead to widespread adoption of new shots when they become available.
What are the “next-gen” vaccines under development?
Next-gen COVID-19 vaccines generally fall into two categories: nasal vaccines that would provide better protection against infection, and pan-coronavirus vaccines that would provide better protection against new variants.
Nasal vaccines basically deliver immunity with a spray into the nose, rather than a shot in the arm. This type of vaccine already exists for other common viruses, like the flu. They’re easier to receive for people wary of needles, but they also have a big advantage for the immune system: these vaccines boost immunity in the nose, mouth, and upper respiratory tract, which are the main places where the coronavirus typically infects people. With a nasal vaccine’s help, the immune system is better poised to fight off the virus at infection, rather than fighting off severe symptoms after someone is already infected.
Pan-coronavirus vaccines, meanwhile, address the variant challenge. Our current COVID-19 vaccines are designed around the virus’ spike protein, a component on the outside of the virus that helps it break into human cells. But the spike protein is the primary area where the coronavirus mutates; the spike proteins of XBB.1.5.1 or XBB.1.16 are very different from that of the original virus. New pan-virus vaccine candidates are designed around different aspects of the virus that don’t mutate as much, and therefore would remain more protective against new variants.
For more details on why these vaccine options are important and which candidates are now in the pipeline, I recommend reading this Substack post by Eric Topol, the prominent COVID-19 commentator and director of the Scripps Translational Research Institute. Topol has been calling on the Biden administration to support next-generation vaccines for a long time; he’s written extensively on this subject.
Why is a federal program important to advance these vaccines?
Operation Warp Speed was a monumental achievement, probably the most successful aspect of the U.S.’s response to COVID-19. The federal government provided significant funding to pharmaceutical companies, while also assisting with clinical trial development and facilitating collaboration between companies and the FDA. And the first mRNA vaccines were delivered within one year of the pandemic starting.
Project Next Gen will provide a similar boost to the companies working on next-gen vaccines. It’s not going to operate at the same scale as Operation Warp Speed; it received $5 billion in funding, compared to Warp Speed’s $18 billion. Still, that’s a huge chunk of money for companies, and other types of federal support that will be crucial for quickly starting up large clinical trials.
The White House is currently assessing pharmaceutical companies that it may partner with on this initiative, according to reporting by the Washington Post. There’s no clear timeline for Project Next Gen yet, as the government will need to work with specific companies and the FDA to plan trials, but it’ll certainly be much faster than these vaccines would get to people otherwise.
What are the challenges facing Project Next Gen?
While this initiative is great news, its implementation will face a lot of challenges—especially after the new vaccines become available. The federal government’s rhetoric around COVID-19, combined with our now-mostly-dismantled infrastructure for responding to the disease, will present major barriers to getting people vaccinated.
For example, it’s obviously very ironic that the Project Next Gen announcement came in the same week as Biden signed a bill ending one of the federal COVID-19 emergencies. And the timing isn’t just coincidental: the White House and HHS are actually using the emergency’s end to fund this project, moving in money that was previously devoted to COVID-19 testing and other preventative measures.
The administration is basically telling people: “COVID-19 is over, but uh, we might need you to get a new vaccine or two next year so that you don’t die from it.” It’s hard to blame people for not getting the second part of the message.
We’re already seeing this with the Omicron boosters: only 17% of the U.S. population has received one, according to CDC data. Lack of awareness about those vaccines and the many barriers that now exist to get the shots contributed to that low number. Even if Project Next Gen delivers the most effective COVID-19 vaccines possible, a lot more investment would be necessary to actually get them to people.
Deaths in U.S. prisons: Throughout the pandemic, the UCLA COVID Behind Bars Data Project has been a leading source for data on COVID-19 cases and deaths in carceral settings. As COVID-specific data on prisons and jails have become more sporadic, the project recently turned its attention to overall mortality data in these settings. Last week, the UCLA team released a new dataset sharing all-cause deaths in prisons through 2020, which combines data from public reports and records requests. The full dataset is available on GitHub, and a summary of this project’s findings on all-cause mortality was published in the New York Times last weekend.
BIOFIRE syndromic trends data: BIOFIRE Diagnostics is a biotech company focused on diagnostic testing, offering tests for a variety of viruses, bacteria, and other pathogens. The company publishes anonymized test results from its labs on its Syndromic Trends dashboard; this dashboard is a helpful way to get an overview of test positivity for COVID-19 compared to other common diseases. (H/t Force of Infection.)
R&D roadmap for COVID-19 vaccines: The University of Minnesota’s Center for Infectious Disease Research and Policy has published a new report outlining the research and development steps needed for the world to produce coronavirus vaccines that are “broadly protective,” not tied to a specific variant. It includes recommendations for research on virology, immunology, and vaccine technologies, along with information on using animal models and guidance on vaccine policy. Related: the CDC’s Advisory Community on Immunization Practices met this week to discuss COVID-19 and other vaccines.
CDC reports on travel surveillance: Two new studies about COVID-19 among international travelers to the U.S. were published in this week’s CDC Morbidity and Mortality Weekly Report. Both studies describe results from the agency’s Travel Surveillance program, which is a collaboration with biotech company Ginkgo Bioworks and testing company XpresCheck. One report compares traveler test results from before and after the U.S. ended its pre-departure testing requirement for international flights, finding that travelers were much more likely to have COVID-19 after the requirement was lifted. The second report provides results from a pilot program testing airplane wastewater at JFK Airport; this report found that the vast majority of plane samples tested were positive for SARS-CoV-2, and researchers identified a variety of Omicron variants. More work is needed to really get airplane wastewater testing going in the U.S., but it’s good to see early results showing this program’s feasibility.
Early data from XBB.1.5 in NYC: Another notable study in CDC MMWR this week provided analysis from New York City’s health department on Omicron XBB.1.5. The subvariant was first identified in the city in October 2022 (though it may have evolved somewhere else), and quickly spread through the region; it accounted for 81% of sequenced COVID-19 test samples by early January. The NYC health department linked sequencing data with patient outcomes data, finding that people infected with XBB.1.5 were not significantly more likely to be hospitalized or to die from COVID-19 compared to those infected with other variants. In other words, XBB.1.5 appears to not cause more severe disease, based on this report.
Predicting COVID-19 cases based on wastewater results: One more newsworthy study to share this week: researchers at Hokkaido University developed a mathematical model to predict COVID-19 cases based on coronavirus concentration levels in Sapporo, Japan. I’m always on the lookout for studies like this, as wastewater data become increasingly important to track true infection numbers. (Here’s a prior example, from the University of Florida.) Of course, it’s worth noting that the Hokkaido researchers had consistent wastewater and case data from spring 2020 through 2022 to use for their model; for wastewater researchers working in the U.S. now, that consistency is often harder to achieve.
CDC committee recommends adding COVID-19 to childhood vaccine schedule: The CDC’s Advisory Committee on Immunization Practices (ACIP), which makes guidance on vaccination policies, issued a report this week recommending that COVID-19 vaccines be added to the standard childhood immunization regimen. Under the new guidelines, most children ages six months and older should receive two doses of a Moderna or Pfizer vaccine, followed by a bivalent/Omicron-specific booster shot. Immunocompromised children are eligible for additional doses.
KFF’s latest COVID-19 Vaccine Monitor focuses on winter surge: The Kaiser Family Foundation recently released the January 2023 update of its Vaccine Monitor project, which tracks U.S. sentiment around COVID-19 vaccines (and other pandemic topics) over time. In the latest round of surveys, KFF researchers found that about 38% of U.S. adults reported that “their households experienced either COVID-19, the flu, or RSV over the past month or so.” About 46% of adults reported that the news of these viruses made them more likely to take safety precautions. The report also includes data on bivalent booster shot uptake, behavior among immunocompromised people, and more.
New variants have yet to emerge from China, study suggests: A new paper from researchers at the Beijing Center for Disease Prevention and Control, published in The Lancet this week, found that COVID-19 cases in China during November and December 2022 were primarily driven by the Omicron subvariants BA.5.2 and BF.7. Both of these lineages entered China from other countries, rather than evolving during the country’s surge following the end of its “zero COVID” policies. The new paper is good news for global health experts who’ve been worried about new variants emerging from China, though outside reviewers have cautioned that it’s only one small snapshot of cases in the country, according to reporting by POLITICO EU.
Wastewater surveillance has a global health equity problem: Another study that caught my attention this week was a paper from the COVIDPoops19 team at the University of California Merced, summarizing findings from their global wastewater dashboard. The team reviewed wastewater surveillance projects at over 200 universities, 1,400 sites, and 55 countries, and found that monitoring primarily occurred in high-income countries. The researchers also examined open access to data, finding that high-income countries were better at sharing information with researchers and with the public. For wastewater-based epidemiology to reach its full potential, “show us the data,” the team writes in their paper’s abstract.
Microbiome research shows promise for understanding ME/CFS: In one more piece of research news: two recent studies suggest that the gut microbiome could play a role in causing myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), a debilitating chronic disease that often occurs after viral infection. In research projects funded by the National Institutes of Health, scientists found specific changes to gut bacteria that were associated with ME/CFS patients. These changes could potentially be used as biomarkers to diagnose ME/CFS and as starting points for treatment. The new research also has potential implications for Long COVID, as many Long COVID patients meet the diagnostic criteria for ME/CFS.