As fall begins, we’re approaching respiratory virus season—that time of year when viruses like the flu, RSV, common coronaviruses, and adenoviruses all spread readily throughout the Northern Hemisphere. Tracking systems for these viruses may also be helpful for following COVID-19 this fall and winter.
While COVID-19 doesn’t yet follow a predictable, seasonal pattern, its activity has increased with these other viruses in the last couple of years. (Indoor gatherings and travel, particularly around the holidays, lead to outbreaks of all kinds.)
This year, experts anticipate COVID-19 will spread with the colder weather again. But we have fewer systems tracking it than we did during earlier pandemic winters: no more case data, testing and hospitalization data aren’t as comprehensive or reliable, death data are significantly delayed (and more likely than ever to undercount true COVID-19 deaths), etc.
So, people seeking to keep up with disease trends in their areas might find it helpful to look at surveillance sources that include COVID-19 along with other respiratory diseases. The CDC’s FluView dashboard is one major source, presenting data from clinical testing laboratories and healthcare settings that participate in the agency’s regular surveillance programs.
Despite the name, FluView includes data on all viruses that cause cold and flu symptoms, including COVID-19. (In fact, the same lab network that informs this dashboard is also the current source of the CDC’s COVID-19 test positivity data.) FluView is a helpful place to see overall respiratory disease activity for the U.S. as a whole and for particular states and regions. I find the state-by-state map of influenza-like activity particularly useful.
Tracking COVID-19 during fall and winter 2023 is going to be harder than it’s been during prior years. But we aren’t entirely in the dark. The CDC’s respiratory virus surveillance programs are one helpful source to look at, along with wastewater surveillance and the other COVID-specific programs that remain active.
Free at-home tests from the federal government: The Department of Health and Human Services (HHS) and U.S. Postal Service are restarting their program offering free COVID-19 rapid, at-home tests. Starting tomorrow, every U.S. household will be able to order four more tests at covidtests.gov. HHS also announced that it’s buying about 200 million further rapid tests from major manufacturers, paying a total of $600 million to twelve companies. Of course, four tests per household is pretty minimal when you consider all the exposures people are likely to have this fall and winter—but it’s still helpful to see the federal government acknowledge a continued need for testing.
New grants support Long COVID clinics: The HHS and Agency for Healthcare Research and Quality (AHRQ) also announced a new grant program for clinics focused on Long COVID, aiming to make care for this condition more broadly accessible to underserved communities. Nine clinics across the country have received $1 million each, with the opportunity to renew their grants over the next five years. (At least, that’s my interpretation of the HHS press release, which says $45 million in total is allocated to this program.) This is a pretty significant announcement, as it marks the first time that the federal government is specifically funding Long COVID care; funding has previously gone to RECOVER and other research projects.
CDC announces new disease modeling network: One more federal announcement: the CDC’s Center for Forecasting and Outbreak Analytics has established a new program to improve the country’s disease surveillance, working with research institutions across the country. The CDC has awarded $262.5 million of funding to the thirteen institutions participating in this program, which it’s calling the Outbreak Analytics and Disease Modeling Network. These institutions will develop new surveillance tools, test them in small-scale projects, and scale up the successful options to broader public health systems. For more context on the CDC’s forecasting center, see my story for FiveThirtyEight last year.
Testing wildlife for COVID-19: Speaking of surveillance: researchers at universities and public agencies are collaborating on new projects aiming to better understand how COVID-19 is spreading and evolving among wild animals. One project, at Purdue University, is focused on developing a test to better detect SARS-CoV-2 among wild animals. A second project, at Penn State University, is focused on increased monitoring, with plans to test 58 different wildlife species and identify sources of transmission from animals to humans. Both projects received grants from the U.S. Department of Agriculture and involve collaboration with state environmental agencies.
Paxlovid access falls along socioeconomic lines: A new study, published this week in JAMA Network Open, examines disparities in getting Paxlovid. Researchers at the National Institutes of Health analyzed public data on Paxlovid availability as of May 2023. Counties with higher poverty, less health insurance coverage, and other markers of high socioeconomic vulnerability had significantly less access to Paxlovid than better-off counties, the scientists found. Meanwhile, a separate study (also in JAMA Network Open last week) found that Paxlovid and another antiviral treatment, made by Merck, both remain very effective in reducing severe COVID-19 symptoms. Improving access to these treatments should be a top priority for the public health system.
Undercounted COVID-19 cases in Africa: One more study that caught my attention this week: researchers at York University in Canada developed a mathematical model to assess how many people actually got COVID-19 in 54 African countries during the first months of the pandemic. Overall, only 5% of cases in these countries were actually reported, the researchers found, with a range of reporting from 30% in Libya to under 1% in São Tomé and Príncipe. A majority of cases in these countries were asymptomatic, the models suggested, indicating many people may not have realized they were infected. The study shows “a clear need for improved reporting and surveillance systems” in African countries, the authors wrote.
In the last week, my social media feeds have been full of stories about vaccine access issues. Even though the updated COVID-19 vaccines are supposed to be free—either covered by insurance plans or by a federal program—people keep getting bills. Or their vaccine appointments are canceled unexpectedly. Or they can’t get an appointment at all.
Some news outlets have covered these access challenges, but far more attention is needed. The new vaccines are the U.S. government’s only real strategy to curb a likely COVID-19 surge this winter, now that masks, testing, and other tools are far less available. It is absolutely crucial that as many people get vaccinated as possible, and any barriers to those vaccinations deserve front-page headlines.
The COVID-19 Data Dispatch may not have the reach of an established national media outlet, but with the help of all of you readers, we can help draw more attention to this massive problem. If you have had a hard time getting an updated COVID-19 shot, please share your experience: you can use this Google form, email me, or reach out on social media (Twitter, Bluesky, Mastodon).
You can share your vaccination experience anonymously or attach your name, location, or other details, if you’d like. (There are no required fields on the Google form.) Next week, I’ll publish the responses in a public database on the CDD website. My hope is that this compilation can show how widespread these vaccine access issues are, and can serve as a resource for other journalists who might be interested in covering the problem.
Also, a PSA: if a pharmacy or doctor’s office tries to charge you for a COVID-19 vaccine, remind them that the vaccines are free. You can refer them to the CDC’s Bridge Access Program, which will pay for any vaccinations not covered by insurance.
I have a new story up this week at Science News, describing how the field of wastewater surveillance exploded during the COVID-19 pandemic and is now looking toward other public health threats.
As long-time readers know, wastewater surveillance has been one of my favorite topics to cover over the last couple of years. I’m fascinated by the potential to better understand our collective health through tracking our collective poop—and by all the challenges that this area of research faces, from navigating interdisciplinary collaborations to interpreting a very new type of data to obtaining funding for continued testing.
My story for Science News builds on other reporting I’ve done on this topic and provides a comprehensive overview of the growing wastewater surveillance field, with a particular focus on how research is now going beyond COVID-19. There’s so much potential here that, as I point out in the story, many researchers are asking not, “What can we test for?” but “What should we test for?”
The future of disease tracking is going down the drain — literally. Flushed with success over detecting coronavirus in wastewater, and even specific variants of SARS-CoV-2, the virus that causes COVID-19, researchers are now eyeing our collective poop to monitor a wide variety of health threats.
Before the pandemic, wastewater surveillance was a smaller field, primarily focused on testing for drugs or mapping microbial ecosystems. But these researchers were tracking specific health threats in specific places — opioids in parts of Arizona, polio in Israel — and hadn’t quite realized the potential for national or global public health.
Then COVID-19 hit.
The pandemic triggered an “incredible acceleration” of wastewater science, says Adam Gushgari, an environmental engineer who before 2020 worked on testing wastewater for opioids. He now develops a range of wastewater surveillance projects for Eurofins Scientific, a global laboratory testing and research company headquartered in Luxembourg.
A subfield that was once a few handfuls of specialists has grown into more than enough scientists to pack a stadium, he says. And they come from a wide variety of fields — environmental science, analytical chemistry, microbiology, epidemiology and more — all collaborating to track the coronavirus, interpret the data and communicate results to the public. With other methods of monitoring COVID-19 on the decline, wastewater surveillance has become one of health experts’ primary sources for spotting new surges.
Hundreds of wastewater treatment plants across the United States are now part of COVID-19 testing programs, sending their data to the National Wastewater Surveillance System, or NWSS, a monitoring program launched in fall 2020 by the U.S. Centers for Disease Control and Prevention. Hundreds more such testing programs have launched globally, as tracked by the COVIDPoops19 dashboard run by researchers at the University of California, Merced.
In the last year, wastewater scientists have started to consider what else could be tracked through this new infrastructure. They’re looking at seasonal diseases like the flu, recently emerging diseases like bird flu and mpox, formerly called monkeypox, as well as drug-resistant pathogens like the fungus Candida auris. The scientists are even considering how to identify entirely new threats.
Wastewater surveillance will have health impacts “far broader than COVID,” predicts Amy Kirby, a health scientist at the CDC who leads NWSS.
But there are challenges getting from promise to possible. So far, such sewage surveillance has been mostly a proof of concept, confirming data from other tracking systems. Experts are still determining how data from our poop can actually inform policy; that’s true even for COVID-19, now the poster child for this monitoring. And they face public officials wary of its value and questions over whether, now that COVID-19 health emergencies have ended, the pipeline of funding will be cut off.
This monitoring will hopefully become “one of the technologies that really evolves post-pandemic to be here to stay,” says Mariana Matus, cofounder of Biobot Analytics, a company based in Cambridge, Mass., that has tested sewage for the CDC and many other health agencies. But for that to happen, the technology needs continued buy-in from governments, research institutions and the public, Matus and other scientists say.
During the most recent week of data available (September 3-9), the U.S. reported about 20,500 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 2,900 new admissions each day
6.3 total admissions for every 100,000 Americans
8% more new admissions than the prior week (August 27-September 2)
Additionally, the U.S. reported:
12.5% of tests in the CDC’s surveillance network came back positive
A 5% lower concentration of SARS-CoV-2 in wastewater than last week (as of September 13, per Biobot’s dashboard)
25% of new cases are caused by Omicron EG.5, 24% by XBB.1.6, 14% by FL.1.5.1 (as of September 16)
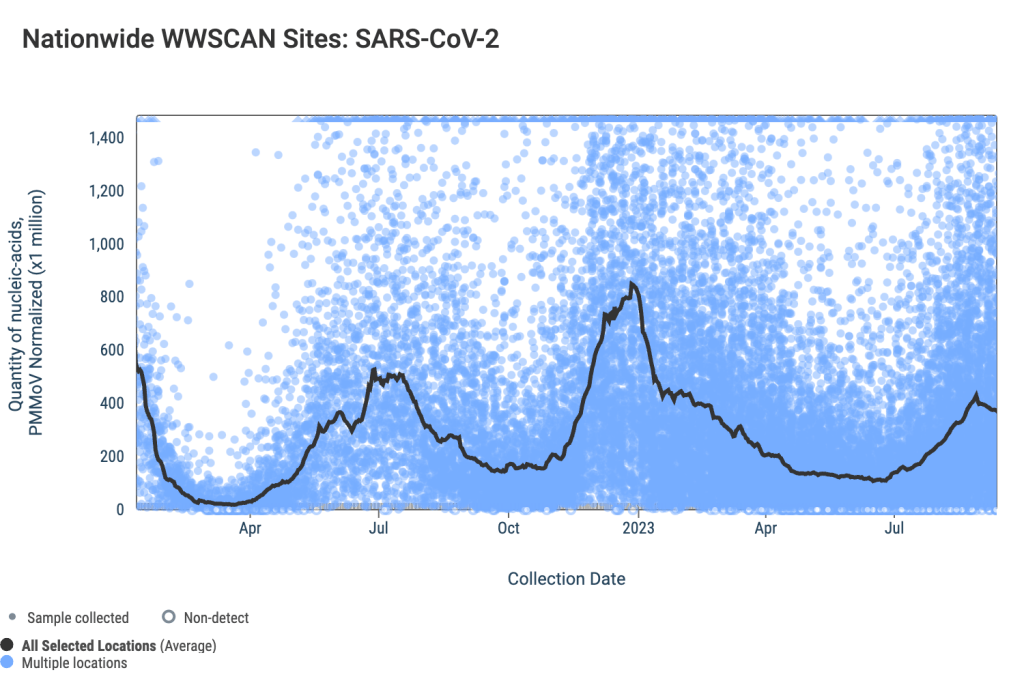
The COVID-19 plateau that I’ve described over the last couple of weeks continues, with wastewater and test positivity data showing that viral spread has slowed in much of the U.S. However, this is likely just a lull before respiratory virus season starts in earnest.
National wastewater data from the WastewaterSCAN project suggest that COVID-19 spread has leveled off in recent weeks, after rising throughout July and August. Biobot Analytics’ data present a similar picture, though the company didn’t update its data this past Thursday (so the most recent numbers are as of September 13).
SCAN and Biobot’s data both show plateaus or declines in all four major regions. But the Northeast and Midwest are reporting more coronavirus in their wastewater sites (at least, in aggregate) than the South and West Coast.
Some sewersheds in the Northeast and Midwest regions have reported increases in recent weeks, while others are leveling off. In Bostonand New York City, for example, most sewersheds report declines or plateaus; while sewersheds in Kansas City and Lawrence, Kansas report upward trends.
To find wastewater data for your region, check the Biobot, WastewaterSCAN, and CDC dashboards. I maintain a list of national, state, and a few local wastewater surveillance dashboards on the COVID-19 Data Dispatch website.
National COVID-19 test positivity is also trending slightly down, according to the CDC’s surveillance network. Test positivity fell slightly to 12.5% in the week ending September 16, from over 14% in the prior three weeks. Walgreens’ testing data show a continued decline in positivity as well.
Hospital admissions for COVID-19 are still going up, according to the CDC—though these data are reported with a significant delay. More than 20,000 people were hospitalized with COVID-19 during the week ending September 9, demonstrating that this disease can still cause severe symptoms. And the CDC has no surveillance data on Long COVID, making that similarly-harmful outcome less visible.
It’s now officially fall, and October marks the start of the respiratory virus season—meaning we can expect more spread of the flu, RSV, and other pathogens along with COVID-19. This is a good time to stock up on high-quality masks, air filters, and other tools that help protect against multiple diseases.
Threads, the new text-based social media platform from Meta (the parent company of Facebook and Instagram), has blocked users from searching about COVID-19 or Long COVID. The block is a harmful choice by Meta, which will make it difficult for health experts, people with Long COVID, and other seeking information to find each other on this platform.
A search function became available on Threads last week, reports Taylor Lorenz in The Washington Post. Health experts and COVID-conscious users tested it out, and quickly discovered that searching for “COVID” or “Long COVID” led to a blank screen with no seach results. Threads instead directed the users to the CDC’s website.
Lorenz received a statement from Meta confirming that the company is blocking these search results:
Meta acknowledged in a statement to The Washington Post that Threads is intentionally blocking the search terms and said that other terms are being blocked, but the company declined to provide a list of them. A search by The Post discovered that the words “sex,” “nude,” “gore,” “porn,” “coronavirus,” “vaccines” and “vaccination” are also among blocked words.
“The search functionality temporarily doesn’t provide results for keywords that may show potentially sensitive content,” the statement said, adding that the company will add search functionality for terms only “once we are confident in the quality of the results.”
It’s unclear what steps Meta is taking to improve the “quality of the results” when users search for COVID-19 information, or when these searches will be available. But for now, experts and advocates who spoke to Lorenz say that the information block is harmful. “Censoring searches for COVID and Long COVID will only leave an information gap that will be filled by misinformation from elsewhere,” said science communicator Lucky Tran.
I personally am not on Threads, and this recent news makes me even more wary of the platform than I’d been already. If you’re looking for a Twitter/X alternative to follow me on, I’ve been trying out Mastodon and Bluesky.
Public comments to the CDC about infection control measures: The People’s CDC, a public health communication and advocacy organization that seeks to fill gaps left by the federal CDC, has published a database of comments about the importance of infection control measures in healthcare settings. These comments were sent to the CDC’s Healthcare Infection Control Practices Advisory Committee (HICPAC), as the committee considers changing the agency’s guidance to be more lenient about preventing infections in healthcare settings. As the CDC has not published comments publicly itself, the People’s CDC “asked people to forward us their comments to HICPAC, and created the People’s Register.” For more details about HICPAC, see this post.
Recommendations for masks, nasal sprays, other tools: In response to last week’s post discussing how nasal sprays may be used to reduce COVID-19 risk, a reader shared this video from RTHM Health, a telehealth clinic focused on Long COVID and related complex chronic diseases. “This video has a section with a good overview of different sprays and the strength of evidence for each one,” the reader wrote. The video also includes recommendations for high-quality reusable masks and respirators, along with other COVID-19 safety tools.
Wastewater surveillance for flu, RSV: A new study, published this week in the CDC’s Morbidity and Mortality Weekly Report, discusses how wastewater surveillance can complement other methods of monitoring the flu and respiratory syncytial virus (RSV). Researchers at Wisconsin’s state health department, the CDC, and other collaborators tracked flu and RSV in three Wisconsin cities’ sewage during last winter’s respiratory virus season. They found that wastewater trends “often preceded a rise” in emergency department visits for these viruses. This study follows other research that has shown wastewater surveillance can be a predictive tool for many diseases, not just COVID-19.
Better understanding coronavirus interactions with human cells: Another recent study, published in the journal Viruses, discusses how SARS-CoV-2 interacts with the proteins in human cells as it replicates. The research team (based at the University of California Riverside) identified a specific cellular process that the virus’ N protein hijacks and uses to copy its genetic material, leading to more coronavirus in the body. These findings could be used to develop new antiviral treatments that target this cellular process, both for COVID-19 and other similar diseases, the researchers said in a press release.
Limitations of prior immunity to COVID-19: One more recent paper that caught my attention: researchers at the University of Geneva in Switzerland studied how prior infection and/or vaccination can impact COVID-19 risk, based on about 50,000 cases and associated contact tracing data from the city of Geneva. The researchers found that both a recent infection and vaccination reduced the risk of getting infected from a close contact sick with COVID-19. But both types of immunity faded within a few months, leading people to remain vulnerable in the long-term. This study suggests that vaccines alone are not sufficient to control the spread of COVID-19; masks, ventilation improvements, and other interventions are needed, the authors argue.
NIH tests universal flu vaccine: Speaking of vaccines: the National Institute of Allergy and Infectious Diseases (or NIAID, one of the National Institutes of Health) announced this week that it’s starting a new trial for a universal flu vaccine. This vaccine, developed by NIAID researchers, can prompt the body to make antibodies against a wide variety of flu strains rather than focusing on one variant. The vaccine has done well in animal studies and is now ready for a phase one clinical trial. NIAID plans to test the vaccine in 24 volunteers, and will follow them closely through immune system testing to see how the vaccine performs.
Data from a CDC presentation suggest that people of all ages, including children, receive a benefit from updated COVID-19 vaccines.
We now have two new COVID-19 vaccines available for this year’s respiratory virus season, one from Pfizer and one from Moderna, which are expected to perform well against current variants. The FDA approved both vaccines this week, and the CDC recommended them for almost all Americans. A third option, from Novavax, may become available in the coming weeks as well.
The federal government aims to present this fall’s shots as the next iteration in routine, annual COVID-19 vaccines—similar to the routine we’re all used to for flu shots. In fact, I’ve seen some news suggesting that the federal health agencies don’t want us to call these shots “boosters,” instead calling them “updated” shots or annual shots.
But this fall’s vaccine rollout is likely to be anything but routine, as it’s the first rollout following the end of the federal COVID-19 public health emergencies. The government is no longer purchasing shots and distributing them for free; now, insurance companies will have to cover the shots.
As a result, many Americans—especially those without health insurance—will have a harder time accessing these vaccines than they have for previous shots. Plus, the federal emergency’s end will make it harder for us to track how the vaccines are performing, as the coronavirus continues to evolve into new variants.
With all of these complications in mind, here are ten key facts and statistics that you should know about this fall’s COVID-19 vaccines.
Pfizer and Moderna’s shots have been approved and recommended for all Americans, ages six months and older.
Despite some debates among scientists about whether younger people really need updated COVID-19 shots, the FDA has approved these vaccines—and the CDC has recommended them— for all age groups. This is important because CDC recommendations are often the basis for insurance coverage, as experts explained at a webinar hosted by the National Press Foundation on Tuesday.
The shots exclusively target XBB.1.5, a coronavirus lineage that is common in the U.S. and globally right now.
According to the CDC’s genomic surveillance program, almost all cases in the U.S. in recent weeks have been caused by XBB.1.5 or related variants from the XBB lineage. Variants like EG.5 and FL.1.5.1 are also XBB descendants, which have been given nicknames to make it a bit easier for scientists to keep track of them.
It’s also important to note that, unlike last year’s boosters, this fall’s shots are monovalent vaccines—meaning they only target XBB.1.5. The shots no longer target the original strain of SARS-CoV-2 that first circulated in 2020. Scientists generally approve of this choice, as the virus has mutated so much since that time.
Moderna’s booster led to a 17-fold increase in antibodies against XBB.1.5 and XBB.1.6.
The vaccine companies presented data to the CDC’s vaccine advisory committee on Tuesday. Moderna’s presentation included results from a study testing its new vaccine against several different variants, using blood samples from people who received the booster.
About one month after vaccination with Moderna’s booster, the participants had about 17.5 times more neutralizing antibodies against XBB.1.5, 16.7 times more against XBB.1.6, 14 times more against EG.5.1, and 10 times more against BA.2.86. Pfizer also presented data, suggesting that their vaccine should similarly perform well against current variants.
The new vaccines should lead to similar side effects as we’re used to from past mRNA shots.
Based on data that the vaccine companies presented to the CDC’s committee, this fall’s Pfizer and Moderna vaccines should lead to similar side effects—headache, fatigue, muscle pain, etc.—as many of us have expected from past rounds of COVID-19 shots. The companies, along with the CDC and FDA, will continue to monitor these vaccines for any safety issues that may emerge as people start to get them.
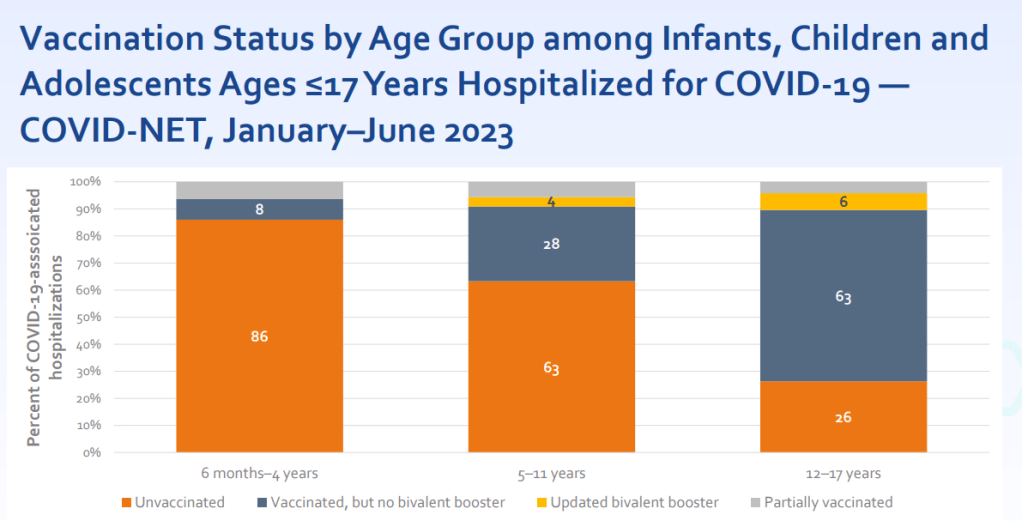
Young, unvaccinated children are at higher risk for COVID-19.
One of the CDC presentations focused on how this fall’s vaccines may benefit young children. Last fall and winter, hospitalization rates were higher for COVID-19 than for the seasonal flu across all young age groups, from infants (under six months) to 12-17 years old. The vast majority of the children hospialized were not vaccinated or hadn’t received last year’s booster.
For some CDC advisory committee members, these data were convincing in suggesting that this fall’s vaccine should be recommended for children, experts told STAT News. Vaccines updated to match current variants have a clear benefit for all age groups.
Long COVID remains a significant risk for Americans across age groups.
Another CDC presentation discussed Long COVID, as one of the potential adverse outcomes of a COVID-19 case. The CDC shared new data from a national survey conducted in 2022, which suggests that 9% of Americans ages 35 to 49 have experienced Long COVID symptoms (defined as symptoms lasting at least three months after a COVID-19 case). Adults ages 50-64 and 18-34 also reported high levels of Long COVID, at 7.4% and 6.8% ever experiencing symptoms, respectively.
Many studies have shown that vaccination lowers risk of Long COVID, though it does not by any means eliminate this risk. While it’s good to see the CDC incorporating Long COVID into its vaccine risk/benefit discussions, much more research is needed to better understand how to prevent this debilitating condition.
A Novavax vaccine is still in the pipeline.
Novavax also presented data to the CDC’s advisors this week, suggesting that its vaccine (also based on XBB.1.5) should perform similarly to the Pfizer and Moderna options. But unlike the Pfizer and Moderna vaccines, Novavax’s has yet to receive FDA approval. The company has said it’s still planning to distribute its vaccine this fall, but it’s unclear when the FDA may authorize it.
Some people are eager to receive the Novavax vaccine this fall, rather than Pfizer or Moderna’s, because this vaccine uses a different mechanism to boost the immune system. It may also lead to fewer side effects than the mRNA vaccine, making it a potentially good option for people who’ve had particularly strong reactions. (I know a couple of readers have sent me questions about this, and aim to do a deep-dive on Novavax in a future issue.)
Only 17% of Americans received last fall’s bivalent booster.
The booster uptake last year was low, according to the CDC. Even among seniors, only 43% received the booster. Can we do better this year?
A POLITICO/Morning Consult poll found that about 60% of respondents said they “probably or definitely” would get this year’s vaccine. (The poll included about 2,000 registered voters from across the U.S.) But it’s likely that access issues could get in the way for many people, as getting this COVID-19 vaccine will be much more challenging than it’s been in past rollouts.
HHS program should provide free vaccines for 25-30 million adults.
The Department of Health and Human Services has officially launched its “Bridge to Access” program, designed to provide free COVID-19 shots to uninsured Americans. Through this program, the HHS is essentially buying a small number of shots and distributing them to pharmacies, federally supported health centers, and other providers. You should be able to view these providers at vaccines.gov, according to the HHS. But I’ll be curious to see how well that actually works.
This year’s vaccine rollout will be much harder to track.
In the past, I’ve written about how the U.S. has failed to monitor breakthrough cases, or COVID-19 infections that occur after someone is vaccinated (and the hospitalizations, deaths, and long-term symptoms that may result). This year, not only are we failing to track breakthrough cases—the U.S. no longer has any national case data at all. We also no longer have vaccination data, as the CDC is not collecting this information from state and local health systems.
So, how will we know how this year’s vaccine rollout goes? It’ll likely be a lot of guesswork, extrapolating from a few state/local health departments, polling data, and other smaller-scale research to estimate how many people are getting vaccinated nationally. This challenge is just another example of the damage that the federal government has done in the last year by dismantling many of its COVID-19 data systems.
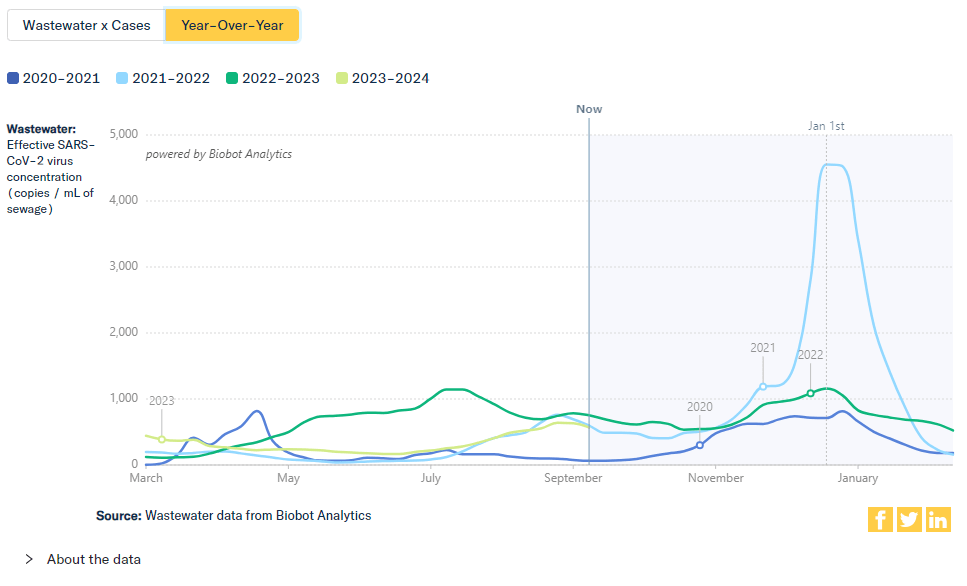
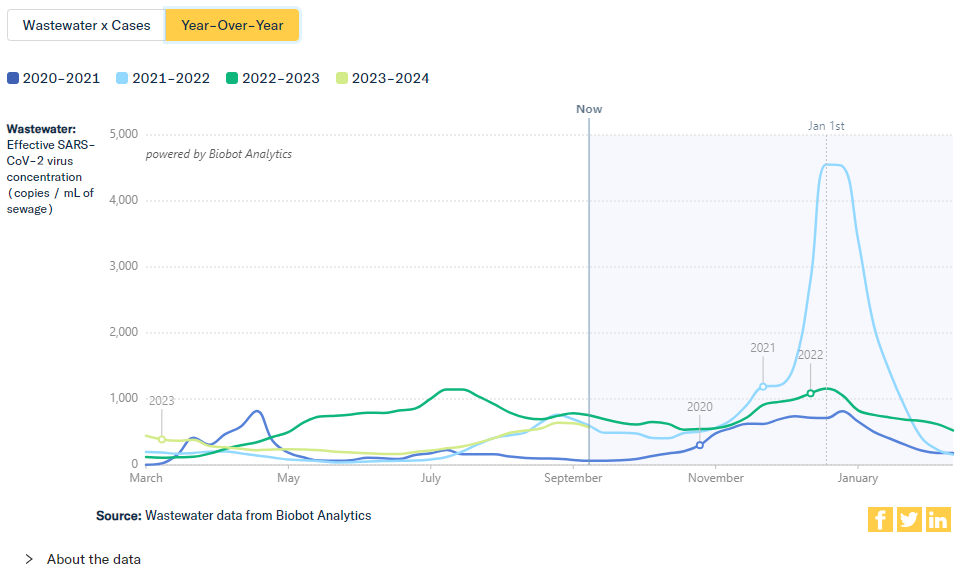
Wastewater data from Biobot suggest that coronavirus levels in the U.S. right now are similar to this time in 2021, during the Delta surge.
During the most recent week of data available (August 27-September 2), the U.S. reported about 18,900 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 2,700 new admissions each day
5.7 total admissions for every 100,000 Americans
9% more new admissions than the prior week (August 20-26)
Additionally, the U.S. reported:
14.4% of tests in the CDC’s surveillance network came back positive
A 10% lower concentration of SARS-CoV-2 in wastewater than last week (as of September 6, per Biobot’s dashboard)
25% of new cases are caused by Omicron EG.5, 24% by XBB.1.6, 14% by FL.1.5.1 (as of September 16)
For the second week in a row, available data suggest that the current COVID-19 surge may be turning around, or at least heading for a plateau. But there’s still a lot of coronavirus going around—and this will likely remain true through the winter respiratory virus season.
Wastewater data from both Biobot Analytics and WastewaterSCAN suggest that coronavirus spread may be ticking down, after two months of increases. Biobot’s national trends show a 10% decline in SARS-CoV-2 levels in wastewater last week, after a 1% decline the week prior. WastewaterSCAN’s trends show a slow decline in the last week, following a slow increase over the summer.
This decline isn’t universal across the country: according to Biobot’s regional data, the South and Northeast are reporting clearer declines in coronavirus spread, while the West is in a plateau and the Midwest is in an increase. Sewersheds in Midwestern cities like South Bend, Indiana, Coralville, Iowa, and Lincoln, Nebraska have reported major increases in SARS-CoV-2 levels in the last couple of weeks, per WastewaterSCAN.
Test positivity data from the CDC’s respiratory virus testing network also suggest that this summer’s COVID-19 surge may be leveling off. About 14.3% of COVID-19 tests in this CDC network came back positive in the week ending September 9, compared to 14.4% and 14.6% in the prior two weeks. (Note: this network includes a sample of testing labs across the country, but is less comprehensive than our testing data were before the federal health emergency’s end.)
Walgreens’ COVID-19 dashboard, which reports test positivity data from the pharmacy chain, shows the positivity rate leveling off as well. The share of Walgreens tests coming back positive went down slightly from 45% in late August to 40% this past week. Walgreens’ dashboard, like the wastewater data, shows that more people are testing positive in the Midwest and West regions.
Hospitalizations for COVID-19 continue to trend up, with the CDC reporting about 2,700 new patients a day during the week ending September 2. While this number may seem small compared to the overwhelmed hospitals we saw in past surges, it’s important to remember that CDC hospitalization data are both delayed and incomplete.
Our most recent data are from two weeks ago, and reporting standards for hospitals are more lenient now than they have been earlier in the pandemic—though the CDC does still collect data directly from facilities across the country.
Variant estimates, also from the CDC, suggest that EG.5 and XBB.1.6 are still the dominant lineages in the U.S. Each accounted for about one in four COVID-19 cases in the last two weeks, while other versions of XBB caused the rest. BA.2.86 hasn’t appeared in the CDC’s prevalence estimates yet, but scientists have detected it in several states, suggesting it could be spreading under the radar.
Biobot’s wastewater data suggest that COVID-19 spread in the U.S. is similar now to this time in 2021, during the Delta surge. If 2023 continues to follow trends from the last two years, we could see transmission plateau in early fall, then rise again during the holiday season. Any lull that we do experience may be a good time to stock up on masks, rapid tests, and other tools to protect yourself and your community.
Wastewater surveillance is re-starting in some Wyoming sewersheds after an earlier iteration of the program ended in December 2021, according to local news reports. This monitoring is a good sign for expanded coverage across more rural parts of the U.S.
In December 2021, however, the testing program ran out of funding and had to scale back. The CDC’s wastewater dashboard includes just four sites in Wyoming that have reported to the National Wastewater Surveillance System in 2023. Data from these sites also appear on the Biobot dashboard, suggesting that they’re being monitored by the company in partnership with local health agencies.
Now, the state’s surveillance program is getting renewed funding, according to a report by Caitlin Tan for Wyoming Public Radio. Tan writes that “some of the larger communities in Wyoming” will soon be testing their wastewater for the coronavirus and other viruses. Data will be posted by the CDC, and the surveillance will continue through at least July 2024, Tan reports.
While the article doesn’t specify how many sites will participate, this is still good news for a state that’s had limited wastewater monitoring over the last two years. I hope to see other more rural states follow Wyoming’s lead.