Coronavirus levels in Boston, Mass. wastewater spiked intensely last week. Chart via MWRA/Biobot.
In the past week (September 24 through 30), the U.S. reported about 330,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 47,000 new cases each day
100 total new cases for every 100,000 Americans
13% fewer new cases than last week (September 17-23)
In the past week, the U.S. also reported about 26,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 3,800 new admissions each day
8.0 total admissions for every 100,000 Americans
6% fewer new admissions than last week
Additionally, the U.S. reported:
2,400 new COVID-19 deaths (350 per day)
81% of new cases are caused by Omicron BA.5; 13% by BA.4.6; 3% by BF.7; 1% by BA.2.75 (as of October 1)
An average of 400,000 vaccinations per day
Official COVID-19 numbers continue to drop nationwide, with case counts down 13% and new hospital admissions down 6% this week compared to the prior week. Still, signals from wastewater suggest this is no time to let our guard down, especially if you live in the Northeast.
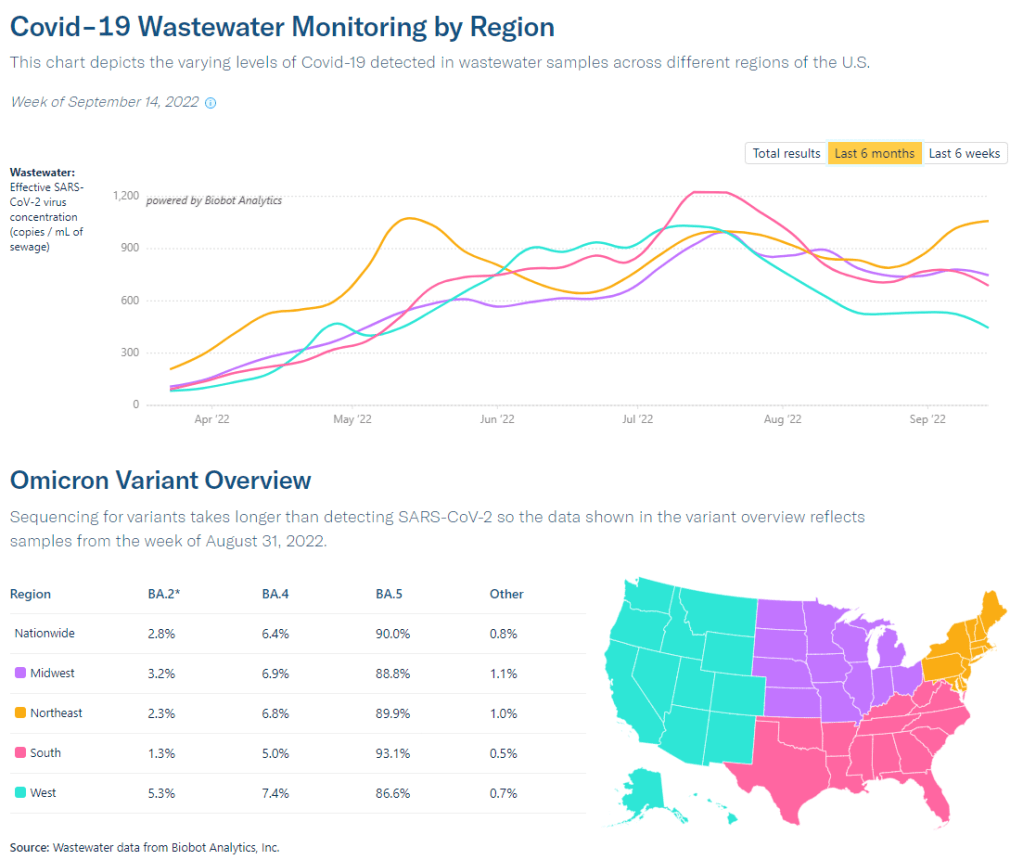
Biobot’s wastewater surveillance dashboard is back this week (after a one-week hiatus). Nationally, this surveillance suggests coronavirus transmission is at a high plateau close to what we saw during early fall of last year, before Omicron hit. The Northeast is driving that recent trend, with an overall coronavirus concentration twice as high as the concentrations reported in other regions.
This region remains a hotspot for Omicron BF.7, the subvariant of BA.5 that could be the U.S.’s next dominant lineage. Nationwide, BF.7 is slowly competing with BA.5: it’s grown from causing about 1% of new cases to 3.4% over the last month, according to CDC estimates. BA.4.6 also continues to grow, while BA.2.75 has remained relatively constant.
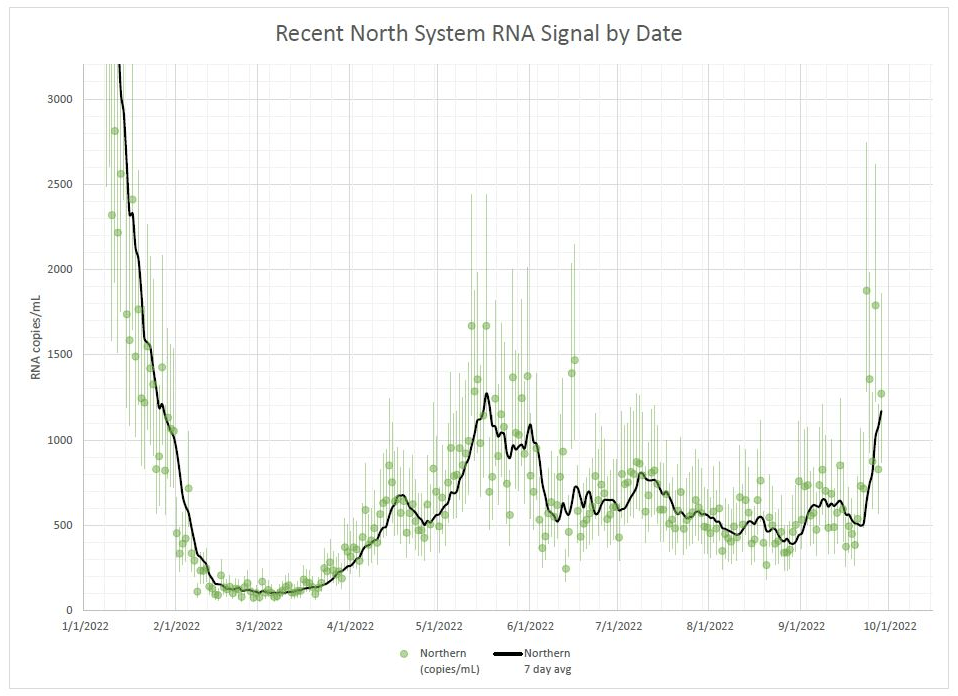
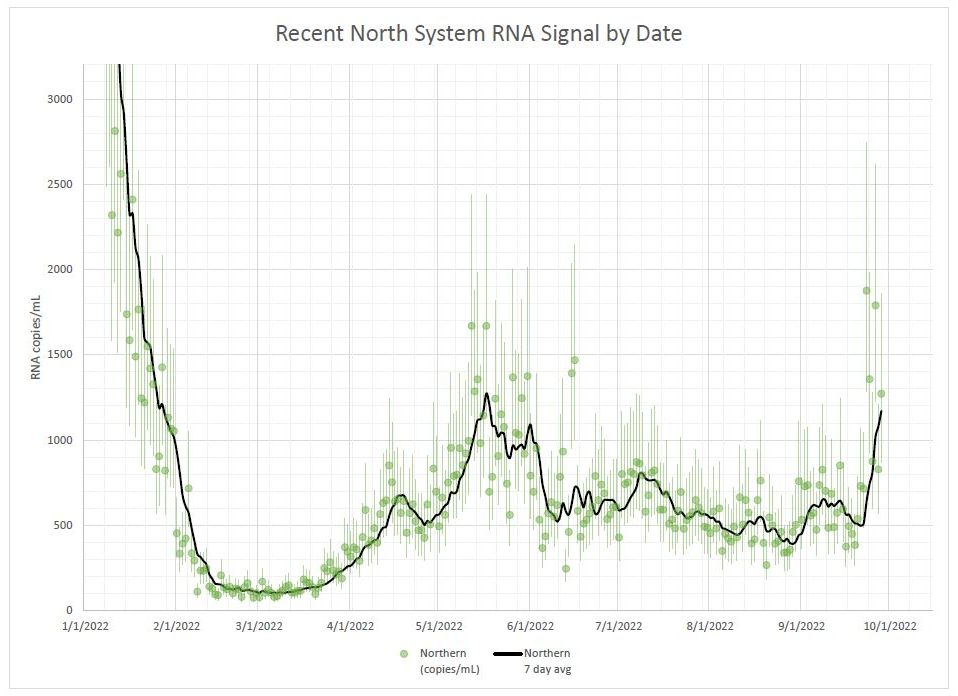
Within the Northeast region, Boston stands out: the city’s wastewater surveillance program (run by Biobot) reported a major spike last week. And by major spike, I mean an increase of more than 100% week-over-week, according to the city’s public health department. “This spike in our wastewater concentration is of great concern and another reminder that the pandemic is far from over,” said Dr. Bisola Ojikutu, Boston’s public health commissioner, in a press release.
Wastewater spikes typically precede case spikes by a couple of weeks, though we’ll have to see whether the significant drop in PCR testing in recent months changes this pattern. Either way, this is a good time to get a booster shot (more on boosters below), stock up on masks and rapid tests, and start planning safety measures for the holidays.
Boston is running vaccine clinics in response to this potential new surge, and the city public health department “recommends” masking indoors. But any further mitigations are likely out of the question, even though they could have a huge impact.
If you went to check Biobot’s COVID-19 wastewater dashboard this week, you may have noticed that the company hasn’t updated its data since September 14.
Biobot’s website doesn’t provide an explanation for the lack of updates, but you can find one on another source: the wastewater data page run by the Massachusetts Water Resources Authority (MWRA), covering the greater Boston area. As Biobot was founded in Boston (by scientists at the Massachusetts Institute of Technology), the city is one of Biobot’s longest-running COVID-19 sampling sites.
As of September 25, a note on the MWRA page reads: “Biobot will be closing their lab next week for a company retreat. We don’t expect any data updates between 9/18/2022 and 9/25/2022. They expect to catch up to the normal posting schedule by 9/27/2022.”
It seems logical to assume this lab closure also applies to the company’s national dashboard.
Now, to be clear, I have nothing against Biobot for taking a company retreat; anyone working in public health deserves a break sometimes, and I hope the retreat is productive for the company’s staff. But when a private company represents the best source for a crucial pandemic-tracking metric—as Biobot is able to provide unified, national and regional estimates better than the CDC can—even a week-long break can be a problem for people who rely on these data.
Ideally, there should be enough public health funding going around that everyone working in wastewater surveillance can take all the breaks they need without disrupting data systems. This is just a small example of a much bigger issue.
CDC adds data on new booster shots: The latest addition to the CDC’s COVID Data Tracker is the Omicron-specific, bivalent booster shots, authorized a couple of weeks ago. So far, the CDC has only provided a total count of Omicron booster recipients (4.4 million, as of September 21) and incorporated these boosters into total counts of Americans who’ve received “first” and “second boosters. A note at the top of the dashboard explains the CDC is working to provide more granular data about the new boosters as separated out from past boosters.
Evidence Commons (ASU): Researchers at Arizona State University’s College of Health Solutions have compiled this detailed dashboard of scientific publications related to COVID-19 tests, supported with funding from the Rockefeller Foundation. The dashboard incorporates information from over 3,000 papers, sorted by the type of test under study, methodology, analysis location, and more. It’s a helpful tool to sort through diagnostic details that are often buried in technical documents.
Helix announces new CDC partnership: Speaking of testing, the viral sequencing and population genomics company Helix announced this week that it has an “extended agreement” with the CDC to sequence coronavirus samples for the agency’s analysis. While Helix has been working with the CDC on variant tracking for some time, the new partnership extends this important effort: Helix (and research partners) will sequence over 3,000 coronavirus samples per week for the next year, “with the option to double the number of samples during surge moments,” according to the company’s press release.
Pathogen Genomics Centers of Excellence: The CDC has also directed new surveillance funding to five state health departments that will test out new genomics technologies and respond to infectious disease outbreaks. These five departments—Georgia, Massachusetts, Minnesota, Virginia, and Washington—are receiving $90 million over the next five years; the funding came out of $1.7 billion allocated for genomic surveillance in the American Rescue Plan. I’m glad to see this sustained funding going beyond COVID-19, though I wish more than five states were getting the money!
Long-term nervous system damage from COVID-19: Ziyad Al-Aly and his team at the Veterans Affairs St. Louis Healthcare System have published a new paper on long-term impacts from a COVID-19 infection. The study used a large dataset of electronic health records from a national VA database, including 154,000 people with COVID-19 and over five million controls. COVID-19 patients had an elevated risk of strokes, cognition and memory problems, seizures, mental health disorders, encephalitis, and more. While the VA population isn’t the best representation for the U.S. population as a whole (it skews older and male), the study still provides evidence for long-term neurological complications from COVID-19.
Long COVID estimates in Europe: And one more piece of Long COVID news for this week: the World Health Organization’s European division has produced new estimates on Long COVID for the continent. Between 10% and 20% of COVID-19 cases in Europe have led to mid- or long-term symptoms, the WHO found, impacting up to 17 million people. The study also found women are more likely to develop Long COVID.
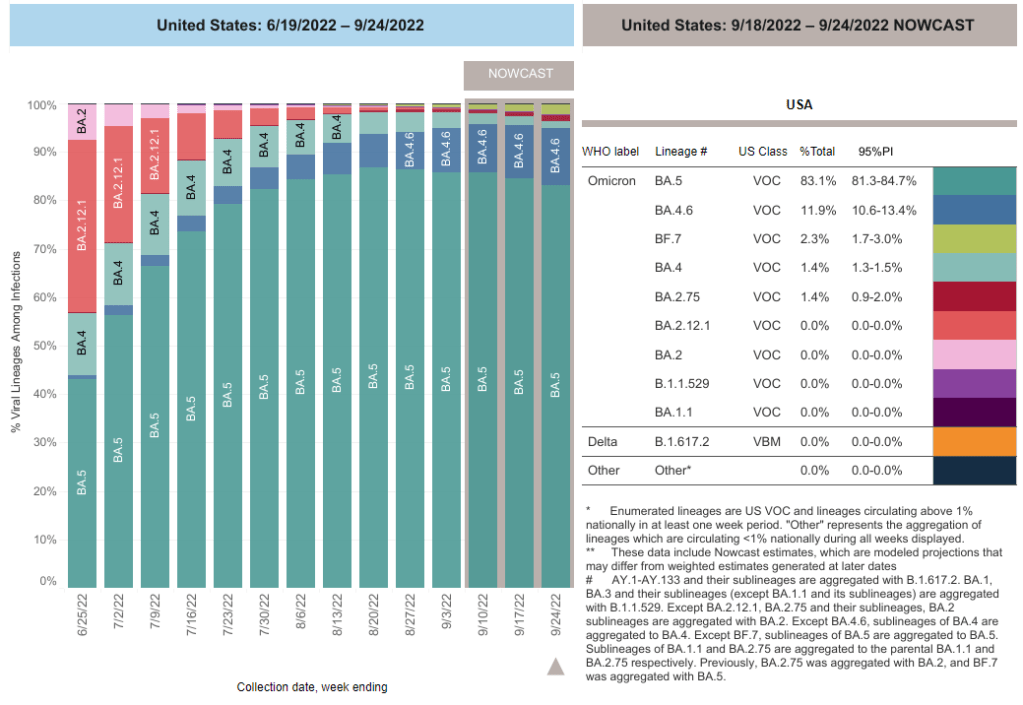
BF.7 (shown here in light green) is among the Omicron subvariants starting to push out BA.5. Chart via the CDC.
Omicron BF.7, an offshoot of BA.5, is the latest subvariant to raise red flags among experts tracking COVID-19 in the U.S.
This week, BF.7 passed BA.2.75, another worrying lineage, in the CDC’s prevalence estimates: the CDC found that it caused about 2.3% of new cases nationwide in the week ending September 24. It’s most prevalent in the Northeast right now: in New England, it caused almost 4% of new cases last week, the CDC estimates.
BF.7 has an additional spike protein mutation compared to BA.5, CDC spokesperson Jasmine Reed told CBS News last week. The agency is concerned that this “genetic change” could lead to Evusheld, an antibody drug used by immunocompromised people, becoming less effective. It could also contribute to a new wave of reinfections, as we’ve seen with other Omicron subvariants in the last few months.
“The same growth advantage in multiple countries makes it reasonable to think that BF.7 is gaining a foothold,” and that it’s potentially more transmissible than parent BA.5, Ray said. Children of variants “don’t grow relative to their parent unless they have an advantage.”
We have relatively little data on BF.7 so far, but it’s worth monitoring closely in the coming weeks.
Long COVID and ME/CFS patients protest in front of the White House, telling Biden that the pandemic is not over and demanding action on their conditions. Image courtesy of ME Action.
“The pandemic is over,” Biden said, while walking through the Detroit Auto Show with 60 Minutes correspondent Scott Pelley. “We still have a problem with COVID. We’re still doing a lot of work on it. But the pandemic is over. If you notice, nobody’s wearing masks, everybody seems to be in pretty good shape.”
Most of the debate and dissection of this interview has focused on Biden’s statement that the “pandemic is over.” Is it, actually? (Epidemiologists say no.) Does he have the authority to declare it over? (No, that’s a job for the WHO.) Was his statement just reflecting what most Americans are already thinking? (Depends on who you call “most Americans.”)
See, I think the key part of Biden’s quote here actually comes at the end: “everybody seems to be in pretty good shape.” Seems to be is doing a lot of work here. In the interview, Biden is strolling through the auto show, through groups of unmasked people looking at car exhibits.
He is not actually talking to these bystanders, asking them whether they’ve lost loved ones to COVID-19, lost work during the pandemic, or faced any lingering symptoms after catching the virus themselves. Biden also isn’t considering the people who were excluded from this auto show: the Americans who were left disabled with Long COVID, and those still taking safety precautions due to other health conditions.
Images of the auto show, like those of packed indoor restaurants or maskless stadiums, seem to suggest that, yeah, Americans no longer care about COVID-19. But there are plenty of other images that don’t make it into high-profile media settings like Biden’s interview.
Today, I invite you to consider a few of the images that Biden isn’t seeing. Here are 12 statistics showing how the COVID-19 pandemic continues to have a massive impact on Americans:
At least 400 Americans are dying with COVID-19 every day, about 47,000 deaths total between June and September 2022. Daily death data tend to be underestimates, because it can take weeks to process death certificates (and numbers are often retroactively edited up). But we can still see that hundreds of people are dying each day. As Sarah Zhang points out in The Atlantic, this is several times the threshold experts set in early 2021 for calling the pandemic at an end.
About 25,000 people are currently hospitalized with COVID-19 cases. Yes, many of the people included in this statistic probably entered the hospital for another reason, then tested positive as part of routine screening. But incidental coronavirus infections still put pressure on the hospitals caring for these patients, and can intersect with a wide variety of other health conditions, potentially causing long-term issues for patients.
About 7.6% of adults are currently experiencing some form of Long COVID, as of early August. This estimate, which I pulled from the Census and CDC’s Household Pulse Survey, rises for certain demographics: almost 10% of women, 11% of transgender adults, 11% of adults with less than a high school diploma, and 15% of adults with a disability are currently experiencing Long COVID.
Hundreds of Long COVID and ME/CFS patients protested at the White House and online on Monday. Biden’s statement coincidentally landed the night before a planned protest, in which patient-advocates called for the president to declare a national emergency around Long COVID and ME/CFS. The protest was covered in the New York Times,MedPage Today, the BMJ, and other outlets.
Long COVID and ME patients are at the White House calling for action on these conditions! Chants I've heard on the livestream include: "No treatment, no peace, we won’t ever cease," "Too sick to chant, funding now." #MillionsMissingpic.twitter.com/phJiTzgwzm
19 patients, patient-advocates, and experts testified at a New York City Council hearing about Long COVID and gender on Thursday. Long COVID patients and those with related conditions (like ME/CFS and HIV) talked about dismissals from doctors and inability to return to their pre-COVID lives. They called for more comprehensive medical care and other forms of financial and social support for patients. I covered the hearing for Gothamist/WNYC.
About 2.5 million adults were recently out of work due to a COVID-19 case, either because they were sick themselves or were caring for a sick person. Another 1.6 million adults were out of work due to concern about getting or spreading COVID-19. These statistics come from the most recent iteration of the Household Pulse Survey, conducted from July 27 to August 8, 2022.
About 2.2 million adults were recently laid off or furloughed due to the COVID-19 pandemic. Another one million had their employers go out of business due to the pandemic, and 900,000 had their employers close temporarily due to COVID-19. These data are from the same Household Pulse Survey.
Over 50 million adults experienced symptoms of anxiety for at least half the days in the last two weeks, at the time of the most recent Household Pulse Survey. Almost 40 million adults experienced symptoms of depression for at least half the days in the same two-week period.
Over 80% of Americans still support the federal government providing free COVID-19 vaccines, treatments, and tests to anyone who needs them, according to an Axios-Ipsos poll conducted in early September. A past iteration of that poll, from March 2022, found that 74% of Americans reported they were “likely to wear a mask outside the home if COVID-19 cases surge again in their area.”
About 3% of Americans, or around 12 million people, are immunocompromised and still have reason to take intense COVID-19 precautions. Immunocompromised people have been eligible for extra vaccine doses, but are still more vulnerable to both severe COVID-19 symptoms and Long COVID.
2.5 billion people worldwide still haven’t been vaccinated, according to estimates from Our World in Data. Bloomberg’s vaccine tracker estimates that, at the current pace of first doses administered, it will take another 10 months for just 75% of the global population to have received at least one COVID-19 shot. As long as COVID-19 continues to spread anywhere in the world, new variants can be a threat everywhere.
In the past week (September 17 through 23), the U.S. reported about 380,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 54,000 new cases each day
116 total new cases for every 100,000 Americans
11% fewer new cases than last week (September 10-16)
In the past week, the U.S. also reported about 28,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 4,000 new admissions each day
8.5 total admissions for every 100,000 Americans
10% fewer new admissions than last week
Additionally, the U.S. reported:
2,400 new COVID-19 deaths (350 per day)
83% of new cases are caused by Omicron BA.5; 12% by BA.4.6; 2% by BF.7; 1% by BA.2.75 (as of September 24)
An average of 300,000 vaccinations per day
Nationally, official COVID-19 case counts continue to decline: reported cases are down about 11% last week compared to the prior week, while new COVID-19 patients in hospitals are down 10%. But signals from wastewater and variants suggest a fall surge may be starting soon.
“Currently, most of the country is reporting moderate to high SARS-CoV-2 levels in wastewater,” CDC officials noted in this Friday’s COVID Data Tracker Weekly Review. For almost 20% of sites, these coronavirus levels are the highest seen since December 2021, the CDC reports. About half the wastewater sites in the CDC’s network are reporting an increase in coronavirus levels and half are reporting a decrease.
Notably, many of the wastewater sites reporting increased coronavirus spread are in the Northeast, a region that’s also a hotspot for Omicron subvariants BA.2.75 and BF.7. BF.7, a new sublineage that evolved from BA.5, is particularly worth watching (more on that below). Overall, the U.S.’s variant composition is slowly shifting from BA.5 to these two subvariants, along with BA.4.6—which caused 12% of new cases nationwide in the week ending September 24.
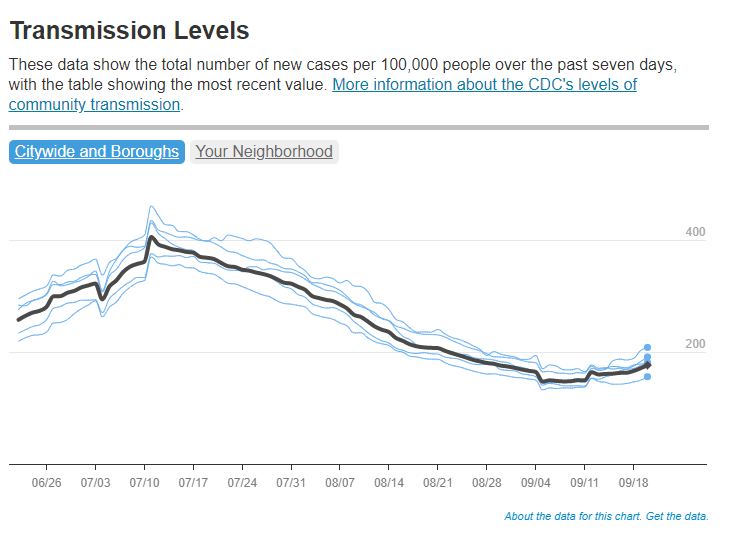
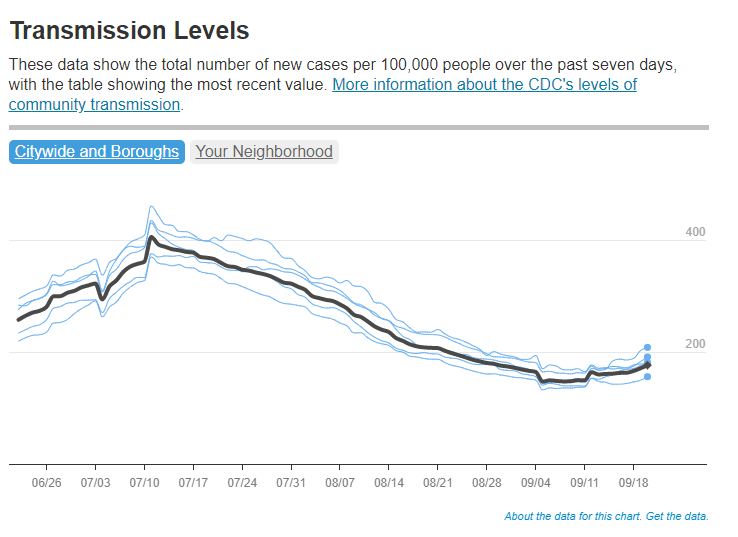
According to the latest Community Profile Report, states reporting significant increases in cases from week to week include Nevada, California, New Hampshire, Kentucky, Massachusetts, New Jersey, New York, and Oregon. In New York City—often a bellwether for new surges—cases have started to tick up slightly, according to the city’s health department, after a long (and slow) decline from July’s summer peak.
Meanwhile, other common respiratory viruses might make a comeback this fall, report Dr. Katelyn Jetelina and Dr. Caitlin Rivers in a joint issue of their newsletters. Data so far on the flu, RSV, rhinovirus, and other viruses we consider part of a normal fall season suggest that children in the U.S. might have a particularly virus-heavy fall and winter—putting more pressure on the healthcare system.
One of the best ways to protect yourself from COVID-19 this fall is by receiving one of the new, Omicron-specific booster shots. According to the CDC, about 4.4 million Americans have received one so far, as of September 21. The new shots have brought our vaccine administration counts to over 300,000 new doses given a day, but that still pales in comparison to the millions administered daily during the spring 2021 campaign.
I received my own booster on Friday at a NYC Health + Hospitals site. Unlike my primary series doses, for which my girlfriend and I had to wait in long lines with hundreds of other New Yorkers, we got our new shots in a small, hard-to-find room tucked away in a small corner of a south Brooklyn hospital campus. This vaccination campaign seems to be almost an afterthought when it deserves primetime attention.
Flyer for the Long COVID and ME/CFS-led protest, happening tomorrow at the White House. Image via ME Action.
Tomorrow afternoon, patient-advocates living with Long COVID and other chronic diseases will be at the White House demanding that the federal government act urgently to address these conditions. ME Action, an advocacy group focused on myalgic encephalomyelitis or chronic fatigue syndrome (ME/CFS), is the leading organization behind the protest.
The protest’s demands include nationwide education on ME/CFS and Long COVID, education specifically for doctors in diagnosing these conditions, funding for research and potential treatments, and economic support for patients.
While the main event will take place in Washington, D.C., organizers are also encouraging people from other parts of the country to participate online. You can learn more about the event here. (I personally plan to watch and cover the protest remotely.)
Patient advocacy around Long COVID and related conditions like ME/CFS has grown mostly remotely over the last two years, so it’s a major milestone for patient groups to converge on the White House in an event like this one. For any journalists interested in covering the protest, feel free to email or DM me for background info, connections to organizers, etc!
A reminder that this protest is happening Monday in DC!! We need as many people involved as possible – please join if you’re able. Masks will be required for the event.
COVID-19’s impact on the workforce: Economists at the National Bureau of Economic Research released a new working paper this week, showing that COVID-19 has “persistently” reduced the U.S.’s labor supply. Using data from the Census’ Current Population Survey, the researchers found that workers who had to take off at least a week from work due to COVID-19 were seven percentage points less likely to still be in the labor force a year later, compared to those who didn’t miss a week. Overall, Long COVID pushed about 500,000 people out of the workforce, the paper estimates. Notably, this estimate is much lower than the analysis from the Brookings Institution published last month; the gap between these two reports suggests a need for more robust data collection on Long COVID and work.
Long COVID prevalence from a population survey: Last week, I shared a new preprint from Denis Nash and his team at the City University of New York, reporting on the results of a national survey used to determine true COVID-19 prevalence during the BA.5 surge. This week, Nash et al. shared another preprint from that same survey, focused on Long COVID. Based on the nationally-representative survey (sample size: about 3,000), the researchers estimate about 7.3% of U.S. adults are currently experiencing Long COVID symptoms—matching estimates from the Household Pulse Survey. One-quarter of those Long COVID patients surveyed reported that their day-to-day life activities were significantly impacted.
Our pre-print on "The epidemiology of long COVID in US adults two years after the start of the US SARS-CoV-2 pandemic". 7.3% of the US adult population (~18.5 million) reported having long COVID by July. What does the epidemiology look like? https://t.co/lbBIDWNe2l [thread]
Lancet COVID-19 Commission shares lessons from the pandemic: The Lancet COVID-19 Commission is an interdisciplinary group of scientists convened by the journal to study the COVID-19 crisis and make recommendations for the future. In the group’s final report, released this week, the scientists focus on “failures of international cooperation” that have contributed to unnecessary illness and deaths. Those failures include delays in acknowledging that the coronavirus spreads through the air, not enough funding for low- and middle-income countries, “the lack of timely, accurate, and systematic data,” and more.
COVID-19 archive of Dr. Fauci’s emails: The COVID-19 Archive is a project aiming to compile digital documents tracing the early phases of the pandemic. Its prototype iteration allows users to search and sort through the early-COVID inbox of Dr. Anthony Fauci, via email records contributed by investigative reporter Jason Leopold. (MuckRock, where I work part-time, is a collaborator on the project, but I’m not personally involved with it.)
U.S. has active circulation of vaccine-derived polio: This week, the CDC and World Health Organization formally announced that the polioviruses spreading in New York state constitute active circulation of vaccine-derived polio. Most other countries that meet this WHO classification are developing nations in Africa, as well as Israel, the U.K., and Ukraine. For more on what exactly “vaccine-derived polio” means and how the disease made a comeback in the U.S., I recommend reading Maryn McKenna in WIRED.
Neurological symptoms associated with monkeypox: Here’s one study in the CDC’s Morbidity and Mortality Weekly Report that caught my eye this week: the agency has identified two cases in which monkeypox patients faced inflammation in their brains (called encephalomyelitis), leading to neurological symptoms. Both patients were hospitalized and required weeks of rehab, including use of walkers. The CDC says these symptoms are rare but worth monitoring, and is encouraging local health agencies to report any further cases.
COVID-19 is still a public health emergency. At the moment, this is true according to both the general definition of this term and official declarations by the federal government. But the latter could change in the coming months, likely leading to more fragmentation in U.S. COVID-19 data.
A reader recently asked me about the federal government’s ability to compile and report COVID-19 data, using our new anonymous Google form. They asked: “Will the CDC at some point stop reporting COVID data even though it may still be circulating, or is it a required, reportable disease?”
It’s difficult to predict what the CDC will do, as we’ve seen in the agency’s many twists and turns throughout the pandemic. That said, my best guess here is that the CDC will always provide COVID-19 data in some form; but the agency could be severely limited in data collection and reporting based on the disease’s federal status.
The CDC’s authority
One crucial thing to understand here is that the CDC does not actually have much power over state and local public health departments. It can issue guidance, request data, distribute funding, and so forth, but it isn’t able to require data collection in many circumstances.
Outside of a public health emergency, CDC has no authority to require states to share data. And even in an emergency, for example, if you look on the COVID Data Tracker, there are systems that have half the states or some of the states. That’s because those were the ones that were willing to share. And that is a very big handicap of doing good modeling and good tracking… Everything you’re trying to measure, for any decision, is better if you measure it in all the states.
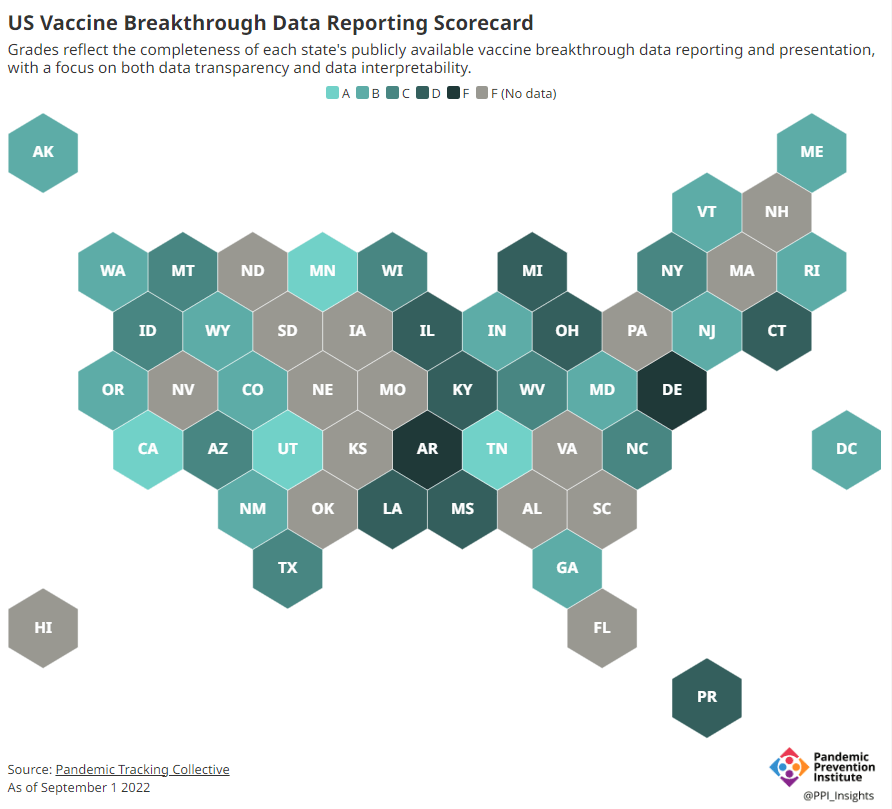
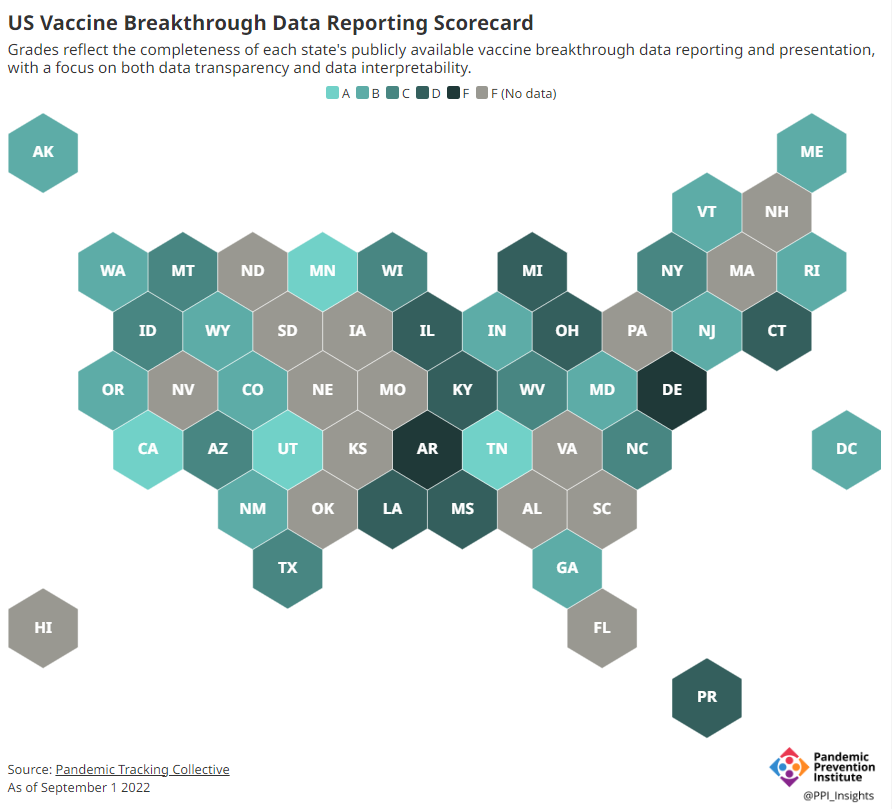
Consider breakthrough cases as one example. According to the Pandemic Prevention Institute’s scorecard for breakthrough data reporting, about half of U.S. states have D or F grades, meaning that they are reporting zero or very limited data on post-vaccination COVID-19 cases. The number of states with failing grades has increased in recent months, as states reduce their COVID-19 data resources. As a result, federal agencies have an incomplete picture of vaccine effectiveness.
Wastewater data is another example. While the CDC is able to compile data from all state and local public health departments with their own wastewater surveillance systems—and can pay Biobot to expand the surveillance network—the agency has no ability to actually require states to track COVID-19 through sewage. This lack of authority contributes to the CDC’s wastewater map still showing many empty spaces in states like Alabama and North Dakota.
During the COVID-19 pandemic, the federal emergency was specifically used to require data collection from state health departments and individual hospitals, POLITICO reported in May. According to POLITICO, the required data includes sources that have become key to our country’s ability to track the pandemic, such as:
PCR test results from state and local health departments;
Hospital capacity information from individual healthcare facilities;
COVID-19 patients admitted to hospitals;
COVID-19 cases, deaths, and vaccination status in nursing homes.
The federal COVID-19 public health emergency is formally controlled by HHS Secretary Xavier Becerra. Becerra most recently renewed the emergency in July, with an expiration date in October. Health experts anticipate that it will be renewed again in October, because HHS has promised to give states a 60-day warning before the emergency expires and there’s been no warning for this fall. That leaves us with a new potential expiration date in January 2023.
CDC officials are seeking to permanently expand the agency’s authority to include this data collection—with a particular priority on hospitalization data. But that hasn’t happened yet, to the best of my knowledge. So, what might happen to our data when the federal emergency ends?
Most likely, metrics that the CDC currently requires from states will become voluntary. As we see right now with breakthrough cases and wastewater data, some states will probably continue reporting while others will not. Our federal data will become much more piecemeal, a patchwork of reporting for important sources such as hospitalizations and lab test results.
It’s important to note here that many states have already ended their own public health emergencies, following a trend that I covered back in February. Many of these states are now devoting fewer resources to free tests, contact tracing, case investigations, public data dashboards, and other data-related efforts than they were in prior phases of the pandemic. New York was the latest state to make such a declaration, with Governor Kathy Hochul letting her emergency powers expire last week.
How the flu gets tracked
COVID-minimizing officials and pundits love to compare “endemic” COVID-19 to the flu. This isn’t a great comparison for many reasons, but I do think it’s helpful to look at how flu is currently tracked in the U.S. in order to get a sense of how COVID-19 may be tracked in the future.
The U.S. does not count every flu case; that kind of precise tracking on a large scale was actually a new innovation for COVID-19. Instead, the CDC relies on surveillance networks that estimate national flu cases based on targeted tracking.
There are about 400 labs nationwide (including public health labs in all 50 states) participating in flu surveillance via the World Health Organization’s global program, processing flu tests and sequencing cases to track viral variants. Meanwhile, about 3,000 outpatient healthcare providers in the U.S. Outpatient Influenza-like Illness Surveillance Network provide the CDC with flu-related electronic health records. You can read more about both surveillance programs here.
The CDC reports data from these surveillance programs on a dashboard called FluView. As you can see, the CDC provides estimates about flu activity by state and by different demographic groups, but the data may not be very granular (eg. no estimates by county or metro area) and are provided with significant time delays.
Other diseases are tracked similarly. For example, the CDC will track new outbreaks of foodborne illnesses like E. coli when they arise but does not attempt to log every infection. When researchers seek to understand the burden of different diseases, they often use hospital or insurance records rather than government data.
One metric that I’d expect to remain unchanged when the COVID-19 emergency ends is deaths: the CDC’s National Center for Health Statistics (NCHS) comprehensively tracks all deaths through its death certificate system. But even provisional data from NCHS are reported with a delay of several weeks, with complete data unavailable for at least a year.
Epidemiologists I’ve interviewed say that we should be inspired by COVID-19 to improve surveillance for other diseases, rather than allowing COVID-19 to fall into the flu model. Wastewater data could help with this; a lot of wastewater researchers (including those at Biobot) are already working on tracking flu and other diseases. But to truly improve surveillance, we need more sustained investment in public health at all levels—and more data collection authority for the CDC and HHS.
Wastewater trends in the past couple of weeks are looking a bit messy, with a potential new surge in the Northeast and plateaus in other regions. Chart via Biobot, retrieved on September 18.
In the past week (September 10 through 16), the U.S. reported about 420,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 60,000 new cases each day
128 total new cases for every 100,000 Americans
16% fewer new cases than last week (September 3-9)
In the past week, the U.S. also reported about 31,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 4,400 new admissions each day
9.3 total admissions for every 100,000 Americans
6% fewer new admissions than last week
Additionally, the U.S. reported:
2,500 new COVID-19 deaths (0.8 for every 100,000 people)
85% of new cases are caused by Omicron BA.5; 10% by BA.4.6; 1% by BA.2.75 (as of September 17)
An average of 25,000 vaccinations per day (per Bloomberg)
Officially-reported COVID-19 cases are still on the decline nationwide this week, as are newly hospitalized patients (a more reliable metric). About 4,400 people with COVID-19 were admitted to hospitals across the country, compared to over 6,000 a day in late July.
These declines may be short-lived, as reopened schools and increased indoor gatherings contribute to new outbreaks this fall. Last week, I warned that Biobot’s wastewater data showed a slight uptick in coronavirus levels across the country; this week’s update shows a continued increase in the Northeast while other regions are in plateaus.
Will the Northeast be the first region to experience a new surge again? It seems feasible, based on data from both Biobot and the CDC—though this region also has better wastewater surveillance coverage than other parts of the country, ABC News reporter Arielle Mitropoulos points out. Boston, one long-running wastewater surveillance location, is reporting high coronavirus concentrations at a level not observed since earlier in the summer.
Nationwide, BA.5 continues to be the dominant variant, causing about 85% of new cases in the week ending September 17 per CDC estimates. But it’s facing competition from newer Omicron subvariants, including BA.4.6 (10% of new cases this week), BA.2.75 (1.3% of cases), and BF.7 (1.7% of cases). As of this week, the CDC is now reporting BA.2.75 and BF.7 separately rather than combining them with other lineages.
BA.2.75, also called Centaurus, is a subvariant from BA.2 that evolved some additional mutations. BF.7 actually evolved from BA.5; its longer name is BA.5.2.1.X. There hasn’t been much reporting yet on BF.7, but it appears to be present in the Northeast—particularly in New England—at higher levels than in other regions. (Possibly another driver of a new surge in this area.)
In addition to BA.4.6, which has now inched past 10%@CDCgov now tracking BF.7 (1.7%) and BA.2.75 (1.3%) variants in its "Nowcast"this week
Overall, while COVID-19 spread in the U.S. is occurring less right now than it did earlier in the summer, the risk of encountering this virus is still pretty high across the country. According to the CDC’s “Community Transmission Level” guidance (pre-February), more than 90% of U.S. counties should require masks indoors.
Instead, we have no masking requirements, increasingly-limited testing, and a booster shot campaign that many Americans do not even know is happening. Between 300 and 400 Americans still die of COVID-19 every day—a number that should be unacceptable—and I fear this number will only go up as we head into winter.
BUMPING THIS because last night I heard from a friend who literally didn't know the new boosters are available to everyone! https://t.co/6tHiaX85UN